Introduction
Today’s society is bombarded with apps such as Instagram which conform to an often unrealistic standard of beauty.1 This could explain why there is such a great desire for perfectionism. Non-surgical cosmetic facial procedures such as botulinum toxin injections and hyaluronic fillers are commonly used to improve the appearance of the face by reducing wrinkles, fine lines and other signs of aging. These procedures involve injecting substances into and under the skin, with proper wound healing being essential to receive optimal results.
Ensuring that the skin heals well after the procedure can help to achieve the desired outcome and minimize the risk of complications.2 Besides the maintenance of aseptic techniques and high adherence to sterile practices before, during and after the procedures,3 the blood flow regulation is another key factor that may be overlooked in some individuals seeking aesthetic procedures.4 The availability of oxygen and the presence of adequate blood flow, with an optimal regulation of blood flow, are important components in the wound healing process.5 Oxygen plays a critical role in the formation of collagen, the growth of new capillaries and the control of infection.6 Unfortunately, some clinicians or aesthetic clinicians are not aware that blood flow can be measured and dysregulation of blood flow can be treated adequately in diverse organs such as the eye,7,8 thus reducing blood flow-related complications that may arise from seemingly minimally invasive aesthetic procedures.
Most aesthetic clinicians are unaware that dysregulation of blood flow commonly occurs in young people who are otherwise healthy. Vascular dysregulation refers to the regulation of blood flow that is not adapted to the needs of the respective tissue.9 Flammer syndrome (FS) is a clinical entity consisting of clinical features caused mainly by dysregulation of blood supply (see www.flammer-syndrome.ch). It can manifest in many symptoms such as cold hands and feet, reduced feeling of thirst, migraines, an altered sensitivity towards various drugs, increased sensitivity to smell, prolonged sleep onset time, increased pain sensitivity and increased levels of systemic oxidative stress.10 The symptoms appear at a young age and weaken as the individual ages. In addition, these individuals commonly have a low Body Mass Index (BMI) and often low blood pressure. Regulation of blood flow can be improved in these individuals using low-dose calcium channel blockers7 while oxidative stress may be reduced by nutrition. Blood flow analysis in the eyes of these individuals shows that the retinal vessels are stiffer and more irregular. Both the capacity of autoregulation, as well as neurovascular coupling, are reduced9,11,12 while retinal venous pressure is increased.13,14 Such dysregulation not only impacts the eyes but virtually all the organs can be involved. Although these individuals are usually healthy, they have a higher risk of developing a variety of diseases such as sudden cardiac ischemia or multiple sclerosis.15,16 For aesthetic clinicians, FS diagnosis is valuable as treatment of FS improves the regulation of blood flow, enhancing better and faster wound healing with optimal results after an aesthetic intervention.
This study aims to investigate the frequency of FS-related signs and symptoms in individuals seeking aesthetic intervention in the Beauty2Go clinic in Lucerne and to study the effect of sex and age on FS prevalence.
Methods
The study population included 207 individuals (189 females, 18 males) to be treated for minimally invasive cosmetic facial procedures (botulinum toxin injections, hyaluronic fillers) at the Beauty2Go clinic in Lucerne between May 2022 and July 2022. All patients received a standardized questionnaire consisting of 15 questions. The participant was asked to mark only one option for each question. The questionnaire had been previously successfully applied to different study populations.17–19 The options on the questionnaire are depicted in Table 1. In total, 13 of the 15 questions have ordinal outcomes and two (Q05 and Q06) have nominal outcomes.
In Table 1, the questions and answer options are listed along with the type of answer (ordinal/nominal). For most items, the highest level of the outcome is an indication of FS. In items Q05, Q06 and Q12, FS is indicated for one of the two levels (Q05: only when I’m cold; yes; Q06: I have a little thirst and drink little; I’m not very thirsty, but I consciously drink more than my thirst demands; Q12: very slim; slim).
To compare the prevalence of the study group with a control group, we retrieved the prevalences from Kunin et al.20 (2018) and Uzunkopru et al.16 (2019), shortened to study 1 and 2 and combined both control groups into a single control group. The group of study 1 (descriptive study) involves healthy individuals who got regular full medical check-ups and were recruited from a Hospital of Dentistry in Russia. The control group of study 2 (exploratory study) are healthy volunteers without any neurological disorders. Our study as well as both retrieved control groups are not randomized.
Statistical analysis
Prevalence of the study population and 95% confidence intervals (CIs) were computed. To compare the prevalence of symptoms with controls, a two-proportional test was used considering the sample size of the combined control in Appendix table 2 and 3. To study the effect of age and sex on ordinal items, an ordinal logistic regression was performed using item outcomes as dependent variables and sex and age as covariates. Probabilities from regression analysis were displayed graphically and coefficients, t-value and 95% CI of the coefficients are available in Table 1 in the Appendix. Statistical software R (version 4.2.1) was used to perform the analysis. In this descriptive study, a p-value of <0.1 was defined as indicative of weak evidence.
Results
In total, 91.3% (189/207) of patients were female and 8.7% (18/207) were male. The mean age was 36.0 years (standard deviation [SD]: 12.1) and the median age was 35.0 years (interquartile range [IQR]: 14.0−67.0). Sample sizes of study 1 and 2 are 20 and 203 individuals, respectively, with a mean age of 33 (minimum: 19, maximum: 67) and median age of 39 (minimum: 17, maximum: 78). Study 1 consists of 65% females and study 2 of 63% (see Appendix Table 2. Prevalences of both studies were combined with weighting factors 9% and 91%.
Table 2 shows the results of the comparison between the study population and the control group. Nine of the 15 symptoms in the study population have a significantly higher prevalence and one has lower prevalence compared to the control. Five signs show no statistical difference to control: Long sleep onset time (Q05), Reduced feeling of thirst (Q06), Headache (Q07), Increased pain sensation (Q10), Tinnitus (Q14). The prevalence of item Migraine (Q08) in the population study is 5.0% lower than in the control group with 12.1%.
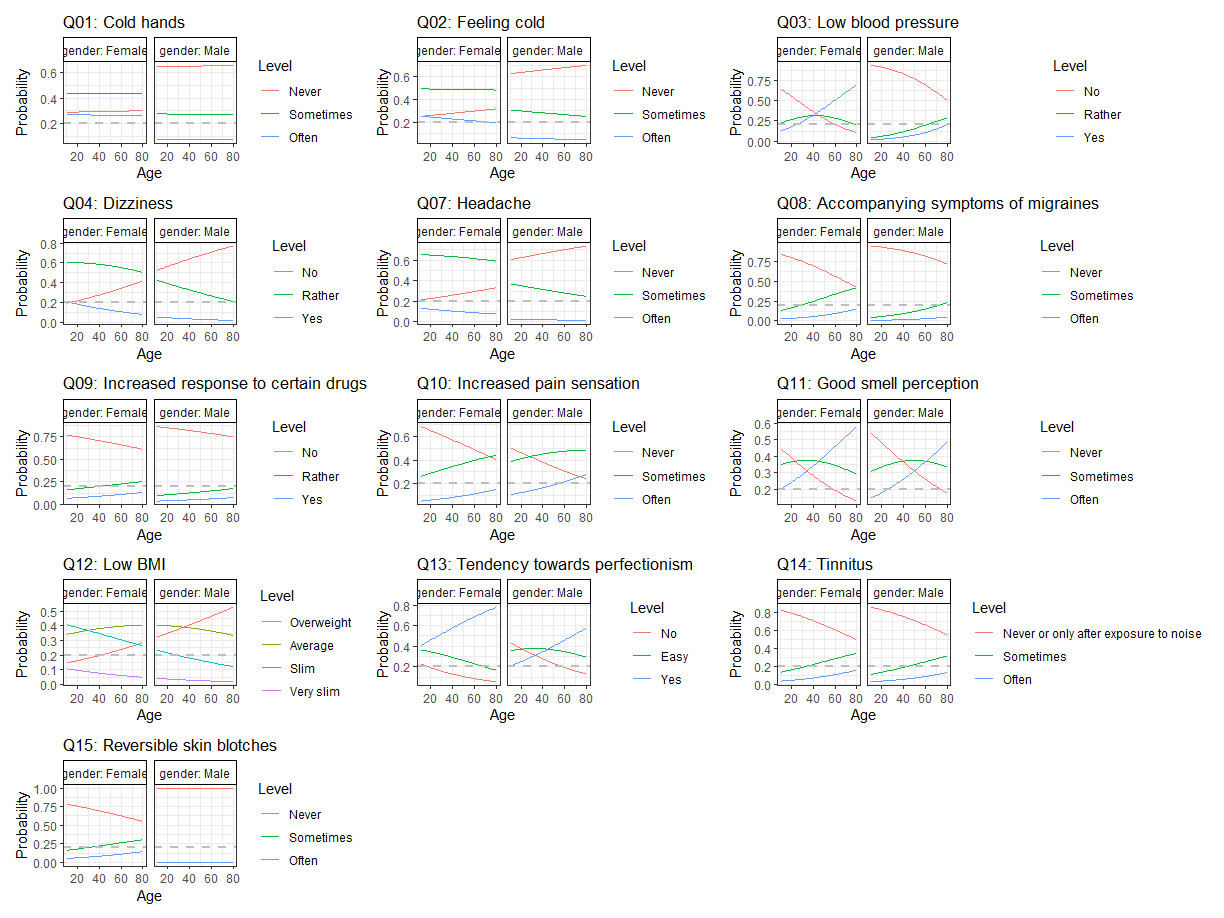
Figure 1 displays the probabilities of different levels (outcomes) of symptoms based on sex and age. The results show that sex has a significant impact on the outcome of item Q01 (cold hand) (p=0.004), with no effect from age (p=0.938). For item Q03 (low blood pressure), both sex and age have an impact (both, p=0.002). Age has a significant effect on item Q11 (good smell perception) (p=0.026), while sex does not (p=0.398). On the other hand, sex has an impact on item Q12 (BMI) (p=0.036), but age does not (p=0.260). Finally, item Q13 (tendency towards perfectionism) may be affected by both age and sex, but the evidence is not conclusive (age: p=0.046; sex: p=0.057). Table 3 summarizes the results from the regression showing the direction of increasing FS symptoms. In five of 13 items with an ordinal scale, the female gender has a higher prevalence for FS than the male gender, adjusted by age. Age increases the prevalence of symptoms in five items.

Discussion
Cosmetic surgery has been and will remain a robust and still growing industry globally,21 with over 30 million surgical and non-surgical treatments worldwide in 2021 alone (de.statistica.com). Particularly women seek out cosmetic procedures at a young age,22,23 while men are still traditionally underrepresented in the cosmetic surgery realm, although they are associated with increasing numbers of aesthetic treatments.24 In our research at the beauty clinic in Lucerne between May 2022 and July 2022, the given data show a distinct distribution of non-surgical interventions of women (91.3%) to men (8.7%), which is consistent with previously reported data. Considering the median age of 36 years, our analysis shows a peak for minimally invasive facial aesthetic procedures, such as botulinum toxin and hyaluronic fillers, in early adulthood. Individuals, especially females show signs of dysregulation of blood flow in the context of FS, although they are usually healthy at these young ages. As the regression shows, the female gender has a higher FS prevalence in several symptoms than the male gender and this may explain why the study group has a higher prevalence in several symptoms compared to the control group (63% females).
There is a great impact of sociocultural factors on how individuals view the ideal standard of beauty today.25 Our society is bombarded with Apps such as Instagram which conform to an often unrealistic standard of beauty.1 This could explain why there is such a great desire for perfectionism or a low BMI. Since patients interested in cosmetic aesthetic procedures are also psychologically engaged in self-optimization,26,27 they may try their best to achieve an even lower BMI, based on body image ideals of social media. Yet, according to the evidence that patients with FS tend to have low BMI,28 fasting periods or even a shift to underweight should be considered as a risk for induction of several severe effects due to vascular dysfunction, such as visual loss or myocardial diseases.15,29
A more recent study by Zubor et al.30 (2017) showed that patients with breast cancer had an increased prevalence of FS symptoms compared to healthy disease-free individuals.30 Knowledge of preoperative risk factors leads to low complication rates and overall satisfactory cosmetic results.31 Since patients with FS have dysregulated blood flow,9 a quick test for FS using a simple questionnaire prior to surgery may improve the chances of a better postoperative outcome.
With the increased use of hyaluronic acid gels and other filling agents for facial cosmetic procedures,32 the role of blood flow circulation has gained attention over the past years. Although associated with a low complication rate, the use of fillers for cosmetic procedures is not without risk.33 Complications range from mild superficial skin irregularities to granuloma formation and vascular occlusion leading to skin necrosis or even blindness.34 A study by Jason W Yu et al.35 (2023), assessing the outcome and the pre-operative risk factors in patients with flap surgery, concluded that cardiovascular diseases were three times more likely associated with complications, therefore careful anamnesis of cardiovascular risk factors prior to surgery is of importance.
Another recent study36 showed the importance of vascular endothelial growth factor (VEGF) for the prevention of skin flap necrosis in plastic and reconstructive surgery. VEGF is a pro-angiogenic molecule that induces neovascularization in ischemic areas, explaining why it is important in wound healing37 itself and especially in case of vascular occlusion. Angiogenesis, which is the creation of new blood vessels from pre-existing blood vessels, has an important role in tissue healing in injured sites by providing oxygen and nutrients to tissues.38 Endothelin 1 (ET-1) is another molecule with a function in endothelial proliferation and growth of smooth muscle cells of the vascular wall.39 ET-1 is a potent vasoconstrictor and higher levels of ET-1 reduce blood flow and may lead to vascular occlusion.40 Data showed that people with FS present with increased plasma levels of ET-1.39,41
Individuals with FS have a higher risk for a variety of diseases such as perioperative visual loss during general anesthesia,42,43 considering the higher sensitivity to local and intravenous anesthetics while using equal doses, vascular occlusions,42,44 multiple sclerosis, retinitis pigmentosa,19 sudden cardiac arrests15 or breast cancer,30 amongst others, which may have an impact on intra- and postoperative outcomes of aesthetic treatments. Golubnitschaja et al.45 conducted a study on “normal BMI” and optimal body weight due to increasing interest in healthy lifestyle. Considering individually determined BMI by our genes, keeping an aggressively low BMI may result in a deficiency of certain nutrients, that are essential for wound healing. As it is known, long periods of calorie restriction have the potential to exacerbate FS symptoms.10 In summary, the data contribute a clearer understanding of an individually based healthy body weight rather than a “standardized normal BMI”, so a stronger focus should be shifted to personalized medicine.
Taken together it is shown, according to our statistical analysis, that there is a significantly higher prevalence of signs and symptoms of FS in our chosen population of individuals seeking cosmetic treatments, However, due to the limitation given by an observational study, more randomized controlled studies are required to assess the concrete relationship between FS in regard of e.g. wound healing and people seeking aesthetic intervention. This knowledge may be useful as patients could be offered prophylactic and preventive vascular treatment.
Conflict of Interest (COI)
All authors have declared that they do not have any conflict of interest and that they have no financial relationships with any organizations that might have an interest in the submitted work.
Author Contributions
MM is the project coordinator who has created the main scientific ideas and hypotheses presented in the manuscript, proofread and made corrections to the manuscript, VF performed the statistical analysis, FL formatted the manuscript, inserted references, helped with illustrations and data collection, FI contributed by expertise in Flammer syndrome and data collection and analysis, KC has recruited patients, analyzed data and helped draft the manuscript. All the authors have read and approved the final manuscript.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Acknowledgments
None.