Abbrevations
-
CBT- i = cognitive-behavioral therapy for insomnia
-
CNS = central nervous system
-
DIMS = difficulty initiating sleep or maintenance sleep
-
GABA = gamma-aminobutyric acid
-
Ghrelin = growth hormone release inducing
-
HbA1c = hemoglobin A1C
-
ICBT- i = internet-based cognitive-behavioral therapy for insomnia
-
T2DM = type 2 diabetes
-
“Z-drug” hypnotics = nonbenzodiazepine hypnotics
Introduction
The average person sleeps 6−8 hours, which is equivalent to one third of the entire life. Shorter sleep duration, as well as disturbed sleep, correlates with health risks and performance impairment.1 Adequate night sleep is characterized by falling asleep quickly, sleeping through the night without repetitively waking up and feeling rested in the morning.2 Sleep research has shown that sleep is essential for mental and physical recovery. Sleep provides the brain with energy,3 activates genes that are important for cellular repair and metabolic processes,4 plays an essential role in memory consolidation5 and the formation and breaking of synaptic connections in the brain.6 In addition, important regulation processes of the fat and glucose metabolism,7 the immune system8 and the long-term maintenance of constant blood pressure9 are sleep dependent. During sleep, arterial blood pressure drops by at least 10% compared to the mean blood pressure while awake (dipping) and is based on a reset (resetting) of the control point of the baroreceptor reflex.10 Lack of sleep leads to an increase in diastolic blood pressure despite reduced sympathetic nervous system activity, which can be interpreted as a resetting of the baroreceptor reflex in the opposite direction.9 According to the new classification of ICD-11 chronic insomnia is defined as difficulty falling asleep and staying asleep with physical impairment during the day several times a week for a period of at least 3 months. For shorter sleep disorders, the short-term insomniac disorder has been included in the ICD-11.
Insomnia and cardiovascular risks
During sleep, the heart rate also decreases due to the change in position and lying quietly. The heart rate continues to decrease as stable sleep is achieved11 but increases again during rapid eye movement (REM) sleep. Disturbed sleep and sleep deprivation are very common phenomena12 that adversely affect the cardiovascular system and are associated with an elevated risk of arterial hypertension,13 atherosclerosis,14 coronary artery disease15 and increased mortality due to heart failure.1
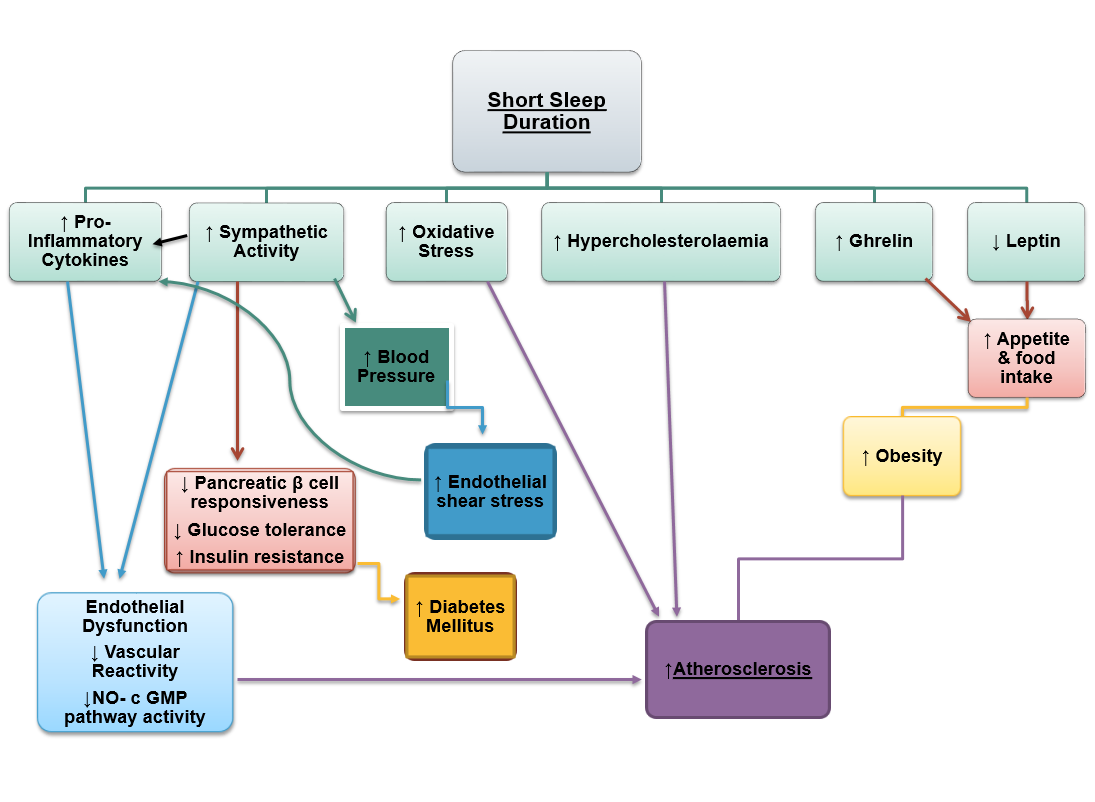
An increased state of inflammation can enhance endothelial dysfunction, which can lead to the development of atherosclerosis. Insomnia exacerbates this condition by inducing oxidative stress and hypercholesterolemia. Apart from this, the activation of the sympathetic nervous system causes a rise in blood pressure, further enhancing endothelial shear stress. Another mechanism whereby the lack of sleep affects cardiovascular health involves a decrease in the concentration of leptin and an elevated ghrelin level, which leads to increased appetite and obesity, further increasing the risk of diabetes mellitus (Figure 1).
Insomnia and sleeping less than 5 hours per night are significantly associated with a remarkably increased incidence of heart attacks, according to a new meta-analysis of 9 cohort studies involving 1.2 million subjects from 6 countries and 3 continents.16 The association is comparable to other heart attack risks, such as diabetes mellitus, smoking and blood pressure. In this study insomnia was defined, according to the current classification at that time, as difficulty falling asleep or staying asleep, sleeping too little or waking up too early without being able to go back to sleep (DIMS = sleep initiation and maintenance disorders).
Insomniac patients are 69% more likely to have a heart attack than the general population, according to this study. The risk of heart attack is 1.56 times greater when sleep duration is ≤5 hours. The study was able to demonstrate a direct connection between insomnia and myocardial infarction, regardless of age, gender, and concomitant diseases such as diabetes mellitus, high blood pressure or dyslipidemia. It was striking that most of the patients examined had no history of a heart attack. A sleep duration of ≥9 hours showed no benefit. The risk was the same for men and women. The results of this meta-analysis do not agree on all points with previous studies. Amongst other things, earlier studies found that not only insomnia, but also non-restorative sleep increases the cardiovascular risk. A prospective study published in 2010 found that a short sleep duration of ≤5 hours per night does not increase cardiovascular risk. The risk was only increased in subjects who slept poorly.17 In insomniac patients, the risk of developing arterial hypertension is more than 3-fold increased.18 A Dutch prospective cohort study with almost 18000 patients, published in the European Journal of Preventive Cardiology, examined the impact of sufficient sleep duration (≥ 7 hours sleep per night) in patients without cardiovascular disease and a healthy lifestyle to reduce cardiovascular risk.19 A healthy lifestyle was defined as adequate physical activity (≥3.5 h/week of sport), healthy nutrition, moderate alcohol consumption and nicotine abstinence. Adequate sleep alone (disregarding the other factors) increases the risk of non-fatal cardiovascular disease by 22% and fatal cardiovascular disease by 43% compared to insufficient sleep. Adequate sleep complementing the healthy lifestyle, which was defined above, reduced cardiovascular risk by 65%. The effect of adequate sleep was comparable to that of not smoking.

Insomnia and diabetes mellitus
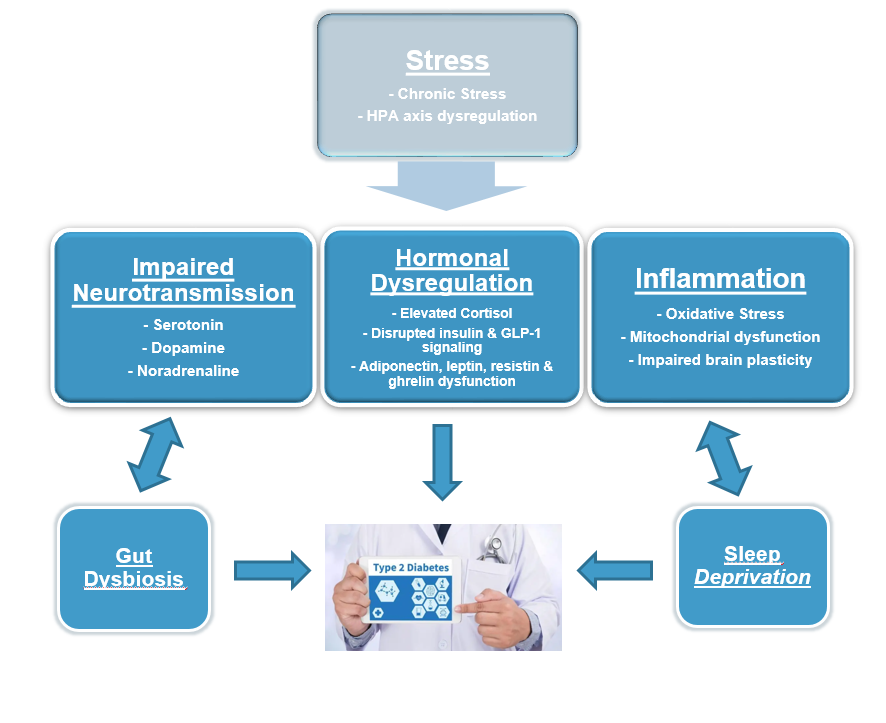
Insomnia tends to be a widespread problem in the population, which can lead to significant comorbidities. Lack of sleep is associated with obesity and arterial hypertension, as well as elevated levels of total cholesterol, triglycerides and hemoglobin A1C (HbA1c). A new multicenter study in Diabetes Care suggests that sleep disorders may play a causative role in the development of type 2 diabetes (T2DM).21 Previous studies22–24 have linked sleep disorders to increased insulin resistance and higher blood sugar levels and thus to a higher risk of T2DM. However, a causal relationship remained unclear due to extrinsic factors (exercise or diet) as well as reverse causality (diabetic nocturia or neuropathic pain) affecting sleep. Data from the UK Biobank and the Meta-analyses of Glucose and Insulin-Related Characteristics Consortium (MAGIC) were analyzed to assess the impact of five patient-reported sleep characteristics (insomnia, sleep duration, daytime sleepiness, napping and chronotype) on HbA1c. The overall population of the above studies was cumulatively 383,367 patients. It turned out that patients with difficulty falling asleep or sleeping through the night had higher HbA1c values than patients who had no or rare sleep disorders. It is worth mentioning that even in non-diabetics, insomnia has led to higher HbA1c levels. The exact pathological mechanisms are still unclear. A dysregulation of several hormones such as evening cortisol, nocturnal growth hormone and ghrelin (“growth hormone release inducing” or “hot hunger hormone”) would be a plausible explanation (Figure 2).
Effects on glucose utilization in the brain, the autonomic nervous system and pro-inflammatory processes are also possible. Lifestyle modification or drug therapy is required to prevent or treat diabetes mellitus.
Associations between type 2 diabetes mellitus and insomnia are already known from earlier studies,22,23,25 although it is not clear whether insomnia leads to higher blood glucose levels or vice versa. Thanks to this new data, there was evidence that insomnia leads to higher blood sugar levels and could therefore play a role in the development of type 2 diabetes.

Therapeutic approaches to insomnia
Sleep disturbances are an extremely prevalent health problem, with about 33% to 50% of adults reporting regular difficulty staying asleep or falling asleep.27,28
The most potent treatment for chronic insomnia is cognitive-behavioral therapy for insomnia (CBT-i).29 This multi-component treatment occurs usually over the course of six to eight sessions (session length may vary between 30 and 90 minutes). Sessions can be delivered in either individual or group format, most often in person or via telehealth once or twice a week. A 2015 meta-analysis of 20 randomized controlled studies of CBT-i for patients with chronic insomnia found average reductions of 26 minutes in time awake after sleep onset and 19 minutes in sleep latency. Sleep efficiency improved by 10% and total sleep by 8 minutes.29 Many sleep disorders are treated unsatisfactorily or not at all due to the lack of treatment options, the resulting costs, and the lack of knowledge about alternative therapies. For this reason, low-threshold offers such as internet-based treatment approaches have been increasingly developed and researched in recent years, as the internet has become popular. Internet-based self-help programs for the treatment of sleep disorders have proven to be effective in various studies. So far, however, these programs have mostly been evaluated as a whole, i.e., participating patients received an entire behavioral intervention package (multi-component intervention) online. The original studies showed a good effectiveness of the online treatment in adult insomnia patients directly after the therapy. The treatment successes achieved were also stable up to 3 years after the end of the therapy, at the follow up measurement point.30–32 For instance, the study by Ritterband et al.31 still showed enormous effect for sleep onset latency, nocturnal wake time after falling asleep and the severity of insomnia symptoms in the follow-up study after one year compared with psychoeducation alone.
Hypnotics could be a therapeutic option for the induction and sleep maintenance in people with insomnia, but only as a short-term therapy and preferably in combination with CBT-i. Hypnotics suppress the central nervous system (CNS) mainly by targeting GABA receptors, which enhance the gamma-aminobutyric acid (GABA) activity, a neurotransmitter that inhibits electrical activity in the brain. The drug classes that are mostly recommended in insomnia- treatment are sedative antidepressants, benzodiazepine-receptor agonists and benzodiazepines.
The nonbenzodiazepine hypnotics (“Z-drug” hypnotics) also act on GABA receptor and are useful in insomnia treatment, owing to their quick onset and short duration of action. The most prescribed Z-drugs include zopiclone, zaleplon, eszopiclone and zolpidem which vary in terms of efficacy and side effects.
A retrospective cohort study with 16064 patients published in June 2023 examined whether the use of hypnotics in patients with insomnia reduces major adverse cardiovascular events, including all-cause mortality and nonfatal major adverse cardiovascular events.33 Treatment with hypnotics (benzodiazepine and Z-drugs) showed higher extended major adverse cardiovascular events but not nonfatal major adverse cardiovascular events. The use of reuptake inhibitors and serotonin antagonists seems to have a protective effect against major adverse cardiovascular events.
A recently approved medication for adults with insomnia whose symptoms have lasted for at least 3 months and have a significant impact on daytime activity is the dual orexin receptor antagonist Daridorexant. The orexin system has an impact on central sleep-wake regulation. A trigger for chronic insomnia can be overactivity of the waking center (hyperarousal). Daridorexant targets the overactive wake system by blocking the binding of orexin to the orexin receptors. The targeted mechanism of action of Daridorexant reduces overactive wakefulness without forcing sleep through sedation.34 The additional benefit of the relatively expensive drug Daridorexant (trade name Quviviq) is controversial, as there are no data that it is superior to already established drugs. Additionally, long-term data are lacking as Daridorexant has been newly approved and therefore the establishment of this drug should be well considered.
Although hypnotics can be an effective short-term treatment for insomnia, some patients experience side effects such as morning hangover, cognitive impairment, and amnestic episodes. In addition, some patients continue to experience sleep difficulties even under sleep medications, leading to higher doses and thus eventual dependence on and tolerance to the drugs.35 Consequently, the use of hypnotics should be evaluated with caution and mainly in combination with face-to-face or internet-based psychoeducation. Furthermore, it should be delivered as a short-term therapy.
Preventive measures in case of insomnia
However, if insomnia cannot be avoided then other measures should be considered. A recent cohort study with over 90,000 people showed that regular physical activity (≥150 min moderate to high intensity) should be aimed at patients with problems falling asleep and staying asleep.36 This was the first study, which used accelerometry to examine sleep duration and the joint effects of physical activity and on mortality risk. An improvement in performance and thus a significantly reduced risk of insomnia-related mortality was achieved. This is explained by the inhibition of the inflammatory state,37 improved glucose metabolism38 and endothelial function.39 Intermediate amounts of exercise and too little sleep led to a 41% raised likelihood of all-cause death. In people with a high amount of exercise, sleep duration was independent to risk of death. The risk of death disappears as soon as the exercise volume increases to moderate or high compared to short sleepers with a low volume of exercise, in whom the risk of death due to heart disease is 69%.36 Studies showed that concurrent health promotion for physical activity and sleep duration is more effective in preventing premature death in middle-aged and older adults instead of focusing on one behavior alone.
Conclusion
In conclusion, primary preventive education for insomnia patients is essential. Patients should be informed about insomnia`s consequences and especially the significantly higher risk of developing a myocardial infarction. Screening for coronary artery disease should also be evaluated in this group of patients. Ideally, people should ensure that they achieve at least moderate physical activity and night-sleep to significantly reduce the cardiovascular risk. However, considering the newest studies, it is indicated that getting sufficient exercise may partially offset the detrimental impact of missing a good night sleep. If restorative and sufficient sleep cannot be achieved, the use of hypnotics can be evaluated as a short-term therapy, though only in combination with CBT-i. Their selection should be, however, very carefully considered, as they can have major adverse effects, such as insomnia, poor function, and poor quality of life. Therefore, long-term therapy with hypnotics is not indicated.
Conflict of Interest
All authors have declared that they do not have any conflict of interest and that they have no financial relationships with any organizations that might have an interest in the submitted work.
Author contributions
SL has made substantial contributions to the conception and design, acquisition of data and analysis and interpretation of data. SL and EB have been involved in drafting the manuscript. EB has given final approval of the version to be published. MH & EB agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Acknowledgements
None.