
Key Message
Fatigue and exhaustion are dominating symptoms of the post-coronavirus (COVID-19) condition.
Clinical trials with Rhodiola rosea extract WS®1375 in patients with various stress loads showed significant improvements of fatigue and exhaustion.
Preclinical and clinical data with Rhodiola rosea extracts provide a promising hint for further investigations in respect to post-COVID-19 fatigue.
Rhodiola rosea extract WS®1375 is a promising candidate against post-COVID-19 fatigue.
The COVID-19 pandemic
Since its outbreak in China at the end of 2019, the global COVID-19 pandemic has impacted the public health, social well-being, and economy globally. Subsequently, more than 600 million people worldwide have been infected by SARS-CoV-2, a new human coronavirus from the Coronaviridae family. As of end of October 2022, the global estimated total number of deaths is 6.6 million (1.1% of infected people). Since 2020, the virus variants Alpha, Beta, Gamma, Delta and since the end of 2021 Omicron coronaviruses are genetically evolved strains of the early 2019 SARS-CoV-2 genome.1,2
Typically, people recover from COVID-19 after one to several weeks. However, a significant proportion of infected subjects experience symptoms lasting for weeks or months after recovery from acute infection. A generally accepted term is “post COVID-19 condition”.3 Long-term symptoms might also be present in persons with only a mild acute illness.3,4 Common symptoms include fatigue, shortness of breath, cognitive dysfunction and generally have an impact on everyday functioning. Symptoms may be new following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time.
Some more specific definitions have been suggested: For example, a recent COVID-19 guideline edited by UK associations and organizations define:
-
“acute COVID-19”: signs and symptoms of COVID-19 for up to 4 weeks.
-
“ongoing symptomatic COVID-19”: signs and symptoms of COVID-19 from 4 weeks up to 12 weeks.
-
“post-COVID-19 syndrome”: signs and symptoms that develop during or after an infection consistent with COVID-19, continue for more than 12 weeks and cannot be explained by any alternative diagnosis.
It usually occurs with clusters of symptoms, often overlapping, which can fluctuate and change over time and can affect any system in the body. A post-COVID-19 syndrome may be considered before 12 weeks while the possibility of an alternative underlying disease is also being assessed. In addition to the clinical case definitions, the term “long COVID” is commonly used to describe signs and symptoms that continue or develop after acute COVID-19. It includes both ongoing symptomatic COVID-19 (from 4 to 12 weeks) and post-COVID-19 syndrome (12 weeks or more).5 It is likely to be difficult for the consulted physicians to arrive at a clear diagnosis in many affected individuals, who may well suffer from an impaired quality of life with a whole spectrum of obvious complaints. Thus, in primary care, a detailed history and physical examination including neurologic, mental, and functional status is recommended.6
Incidence of post-COVID condition
A recent meta-analysis from 15 studies encompassing 47,910 patients showed that 80% of patients develop at least one symptom during follow-up times ranging from 2 weeks to 4 months post viral infection.7 The results of a population-based cohort study with more than 10,000 individuals tested positive for SARS-CoV-2 in Denmark revealed that 13.3% of patients show symptoms for at least 28 days, 4.5% for at least 8 weeks and 2.3% for at least 12 weeks.8 In a meta-analysis of a total of 57 studies with 250,351 COVID-19 survivors, the median proportion experiencing post-COVID-19 condition was 54.0% at 6 or more months.9 The prevalence of post-COVID-19 symptoms is more common after severe courses, but these symptoms might also appear after only mild infections.10 Virus variant appears to be a determinant of post-COVID-19 incidence. In a recent case-control observational study from the UK, 4.5% of omicron cases experienced post-COVID-19 compared to 10.8% of delta cases. However, with the increasing omicron infection rates the absolute number of people with post-COVID-19 will rise.11 The data of this study indicate that the risk of post-COVID-19 depends on the virus variant. Of note, during the severe acute respiratory syndrome (SARS) pandemic in 2002–2004, which led to similar post-acute effects obviously due to the similarity of the two viruses, the prevalence of post-SARS sequelae was estimated to be 10–20%, based on studies with a follow-up of 2 months to 12 years.4
Dominating symptoms of post-COVID conditions
Fatigue is undoubtedly the dominant symptom in post-COVID-19 conditions; however, there is a wide range of additional symptoms. For example, in a meta-analysis of 15 studies with 47,910 patients the most common symptoms were fatigue (58%); other symptoms were headache (44%), attention disorder (27%), hair loss (25%), and dyspnea (24%).7 A different study noted that fatigue is a dominant feature of both acute and post-COVID, with up to 46% of patients reporting fatigue that lasted from weeks to months. In most COVID-19 cohort studies, some authors see persistent fatigue in a significant group of patients, ranging from 13% to 33% at 16–20 weeks post-symptom onset.12 In a cohort study of initially about 1,700 patients with confirmed COVID-19 who had been discharged from a Hospital in Wuhan, China, between January and May 2020, 6 months after acute infection COVID-19 survivors were mainly affected by fatigue or muscle weakness (63%), sleep difficulties (26%) and anxiety or depression (23%).13 A further study conducted 2020 in Norway assessed the prevalence and determinants of fatigue in a population-based cohort of around 450 non-hospitalized patients 1.5–6 months after COVID-19. 46% reported fatigue with the highest prevalence among women.14 In a meta-analysis of a total of 57 studies with 250,351 survivors with ongoing symptoms in 54% at 6 or more months the most prevalent general symptom was fatigue or muscle weakness (median 37.5%); other dominating symptoms were generalized anxiety disorder, general functional impairments and difficulties in concentration (medians of 29.6%, 44.0% and 23.8%, respectively).9 In individuals not requiring hospitalization published studies reported high prevalence of symptoms such as fatigue (30–40%) and persisting dyspnea (10–30%) up to 6 months after SARS-CoV-2 infection. In a patient-initiated survey which recruited individuals from “long COVID” support groups on social media, more than 95% reported fatigue and more than 75% dyspnea.8 Of note, after SARS the prevalence of fatigue was reported to be 19.3% in a meta-analysis.4
Commonalities of post-acute infection syndromes
Many acute infections have been associated with chronic disability in a proportion of patients. These so-called post-acute infection syndromes (PAISs) share similarities irrespective of the causal agent, e.g., Coxiella burnetii, Ebola, Dengue, Polio, SARS, Chikungunya, West Nile Virus, Borrelia, or Giardina lamblia. PAISs are characterized by the main symptoms of exertion intolerance, fatigue, neurocognitive and sensory impairment, flu-like symptoms, unrefreshing sleep, myalgia/arthralgia and other more unspecific symptoms. Many of the PAISs are summarized under the term “fatigue syndromes”. The symptoms of post-COVID-19 condition are similar to those of postinfectious fatigue syndromes following other infectious diseases. In addition, clinical features of PAISs overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). This suggests that there is a high likelihood of common pathogenetic pathways.4
A number of hypotheses on PAIS have been developed:
-
persistent infection or non-infectious remnants of infectious agents in deep tissues that might trigger prolonged inflammatory conditions; shown for Ebola, West Nile virus; SARS-CoV-2;
-
autoimmune reaction; shown for COVID-19 in some patients during acute phase and in post-infection phase;
-
dysregulation of the microbiome, includes reactivation of latent viruses;
-
inability to repair tissue damage; or
-
endothelial dysfunction and microthrombi with consecutive vascular inflammation.4
The symptoms of ME/CFS have been linked to both, exogenous and endogenous agents, including the gastrointestinal microbiome, gut inflammation or the immune system. Several cytokines are correlated with symptom severity of fatigue and cognitive dysfunction and thus they may serve as biomarkers for immune activation.15 Metabolomic studies indicated a generalized impairment in energy production; a hypometabolic state characterized by depressed levels of most metabolites; a redox imbalance with predominance of pro-oxidative processes and reduced generation of the energy source adenosine triphosphate (ATP) and decreased levels of antioxidants; increased levels of inducible nitric oxide synthase (iNOS); autonomic nervous system abnormalities and downregulation of the hypothalamic-pituitary-adrenal (HPA) stress axis.15,16
Such metabolomic alterations might also be interrelated: inflammation can create redox imbalance that, in turn, can damage mitochondrial DNA and membranes. Conversely, mitochondrial dysfunction can lead to inflammation and redox imbalance to damaged tissue.15,17
Pharmacotherapy of post-COVID-19 condition
So far there are no established drug treatments for post-COVID-19 conditions. The effectiveness of early SARS-CoV-2-vaccination in patients with post-COVID-19 conditions is not certain. For the time being, this should only be done in studies.6
One of the drug classes of interest for the treatment of fatigue are the so-called adaptogens. The concept of “adaptogens” dates back to the mid-20th century, when the Russian scientist Nicolai V. Lazarev was commissioned by the Soviet Academy of Sciences to look for a way to increase the body’s own non-specific defense to better adapt to stressful situations and to increase physical and mental endurance and alertness. He coined the term “adaptogens” for this purpose. An adaptogen has a relatively unspecific pharmacological effect and the effect is understood as an increase in the resistance or regulatory power of the organism against biological, chemical and physical factors and also in the case of increased psychological stress.18 In particular, adaptogens have been ascribed antifatigue effects during stress.19 The search for suitable active substances, especially by the pharmacologist I. Brekhman, very quickly focused on herbal active substances, as they were generally well tolerated.18,20,21 Today, the class of adaptogens include only a few herbal active substances, namely preparations from Rhodiola rosea L. (rose root, arctic root), Eleutherococcus senticosus (Rupr. et Maxim.) Maxim. (Siberian or Russian ginseng or taiga root) and Panax ginseng C.A. Meyer (Chinese or Korean ginseng).
Rhodiola rosea or rose root belongs to the plant family of Crassulaceae and is widespread in arctic regions such as Siberia, China, Korea, Scandinavia, Iceland, North America, as well as in mountain ranges throughout Europe and Asia (Figure 1). Rose root has been known as a medicinal plant for various uses since ancient times. Interestingly, it was already taken along by the Vikings for protection against illness during long journeys. In the 1960s Soviet researchers looking for adaptogens developed an interest in the plant. As early as 1975, a tincture was registered as a medicinal product in the Union of Soviet Socialist Republics (USSR), which was used for competitive athletes and cosmonauts.20,22

There has been increasing scientific interest in Rhodiola rosea which is reflected in the rising number of publications in scientific papers. In the European Union (EU), preparations from Rhodiola rosea are recognized as traditional medicines for the relief of stress symptoms such as feelings of tiredness and weakness. Rhodiola rosea extract WS® 1375 is the active ingredient in the product Vitango®. The extract is manufactured from the root or rhizome of Rhodiola rosea L. One film-coated tablet contains 200 mg dry extract of Rhodiola rosea root and rhizome (drug-extract ratio 1.5–5:1, extraction solvent: ethanol 60% [w/w]).
The data from experimental studies available so far suggest that the effect of Rhodiola rosea preparations on stress-associated symptoms is essentially based on two mechanisms. One is the regulation of stress hormones. The effect is mediated by modifications of transcription and signal transmission.22 Secondly, the energy metabolism is activated and the energy carrier ATP is protected. Its increased consumption in stressful situations is slowed down by antioxidant properties and compensated for by activation of mitochondrial ATP synthesis (Figure 2).19,23,24

Mechanisms on cellular level
In an experimental study in the human neuroblastoma SH-SY5Y and the murine hippocampal HT22 cell lines, the effects of Rhodiola rosea extract WS®1375 on neuronal reactive oxygen species (ROS) regulation, bioenergetics, and neurite outgrowth was investigated, as well as its modulatory effect on the brain derived neurotrophic factor (BDNF) pathway. In this experiments stress was induced using the corticosteroid dexamethasone. WS®1375 increased bioenergetics as well as cell viability and scavenged ROS with a similar efficacy in both cell lines and counteracted the respective corticosteroid-induced dysregulation. Additionally, the extract promoted neurite outgrowth and induced an increase in BDNF levels.25
The possible modulation of neuroinflammation was studied in an in-vitro model of corticotropin releasing hormone (CRH)-stimulated microglial cells. Rhodiola rosea extract was able to counteract the neuroinflammatory effect of CRH by inhibiting nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB)nuclear translocation with a mechanism of action involving the modulation of mitogen-activated protein kinase-activated protein kinase 2 (MKK2), extracellular signal-regulated kinase 1/2 (ERK 1/2) and c-Jun n-terminal kinase (JNK), resulting in a reduction of heat shock protein HSP70 expression. Heat shock proteins protect cells from various conditions of stress and thus play an important role in stress response.26
In a study on the protective effects of Rhodiola rosea extract against cellular parameters of fatigue the extract significantly inhibited muscle cell death and ATP reduction caused by hydrogen peroxide (H2O2) damage.27
Animal data
The oral administration of Rhodiola rosea extract in mice improved treadmill running time and blood profiles of glutamic oxaloacetic transaminase, glutamic pyruvic transaminase, lactate dehydrogenase, creatinine, and lactate. Given the above results, the authors considered that Rhodiola rosea extract effectively protects against fatigue caused by strenuous exercise.27
Rhodiola rosea extract activated the synthesis or resynthesis of ATP in mitochondria and stimulated reparative energy processes after intense exercise in rats. In this study, the effects of oral treatment with extracts from Rhodiola rosea and Rhodiola crenulata on the duration of exhaustive swimming and ATP content in mitochondria of skeletal muscles were investigated in rats. Treatment with Rhodiola rosea extract significantly prolonged the duration of exhaustive swimming in comparison with control rats and rats treated with the Rhodiola crenulata extract.23
Another study reported that Rhodiola rosea extract extended both mean and maximum life span of the model organism Drosophila melanogaster. It also found that it lowered mitochondrial superoxide levels and improved protection against the superoxide generator paraquat. The extract did not alter the activities of the major antioxidant enzymes, the superoxide dismutase or catalase, nor did it afford protection against H2O2 or soluble iron. These results suggest a decrease in endogenous superoxide levels as a possible mode of action.28
Rhodiola rosea extract WS® 1375 reduces fatigue and exhaustion – clinical data
Clinical data on WS® 1375 dealing with fatigue and exhaustion in patients with life-stress symptoms, fatigue, and burnout symptoms, respectively, are available from three studies in which a dosage of 200 mg of the extract was applied 2 times per day for 4 to 12 weeks. The inclusion criteria also included exhaustion, lack of concentration, loss of zest for life as well as fatigue. The evaluation of the clinical effect was recorded using specific psychometric questionnaires, such as the Multidimensional Fatigue Inventory 20 (MFI-20), a validated self-report instrument designed to measure fatigue, consisting of 5 subscales of fatigue: general fatigue, physical fatigue, mental fatigue, reduced motivation, and reduced activity.
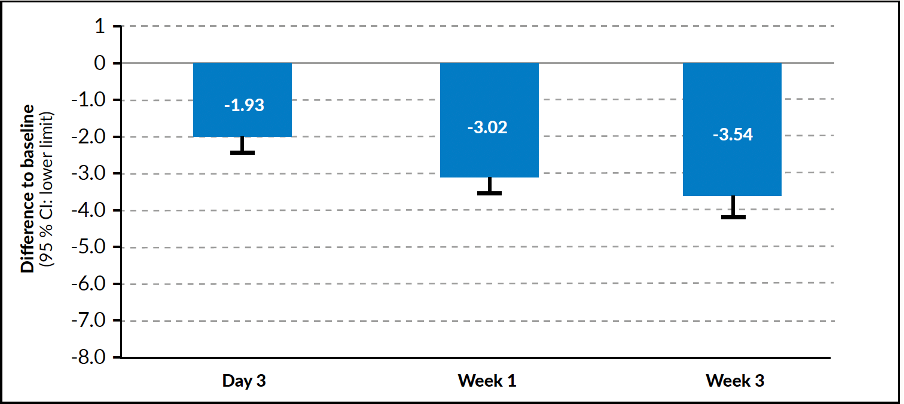
In the first study the therapeutic effects and safety of a 4-week treatment with WS® 1375 in subjects with life-stress symptoms was investigated in a multicenter open-label, single-arm trial. 101 subjects were enrolled in this clinical trial and received the study drug for 4 weeks. Concerning fatigue, improvements were seen in all the MFI-20 subscales (general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation). Clinically relevant improvements were also observed in respect to exhaustion and impairment of concentration and others. The clinical improvements of the latter were significant after 3 days of treatment and continued to increase until study end (Figure 3 shows data for exhaustion).29
_(scaling_fro.png)
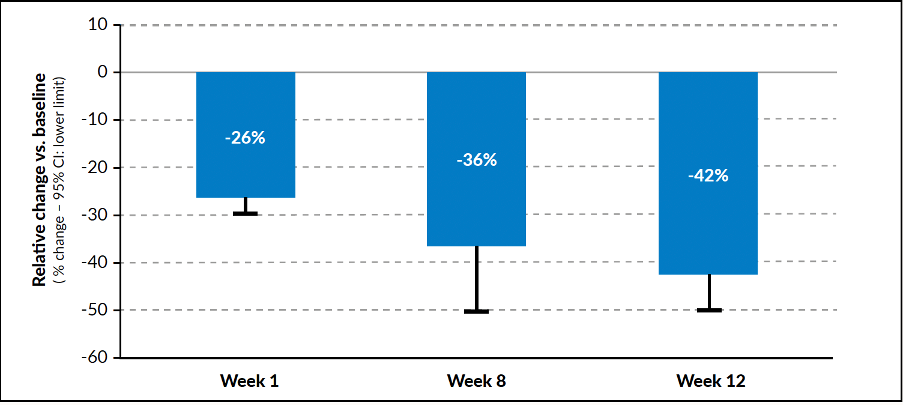
In a further study, conducted as an exploratory, open-label, multicenter single-arm trial, a total of 118 outpatients with burnout symptoms were enrolled and treated for 12 weeks with WS® 1375. Most of the resulting measurements showed clear improvement over time. Several parameters had already improved after 1 week of treatment and continued to improve further up to the end of the study. In detail, all sub-scores of the Perceived Stress Questionnaire (PSQ) as well as the total PSQ global score distinctly decreased between screening and end of the intervention period. The PSQ sub-score “fatigue” improved after 12 weeks of administration of WS®1375 2.4±3.0 (mean ± standard deviation). Exhaustion significantly improved over 12 weeks of treatment, with the greatest change occurring during the first week (Figure 4).30
_(scaling_fro.png)
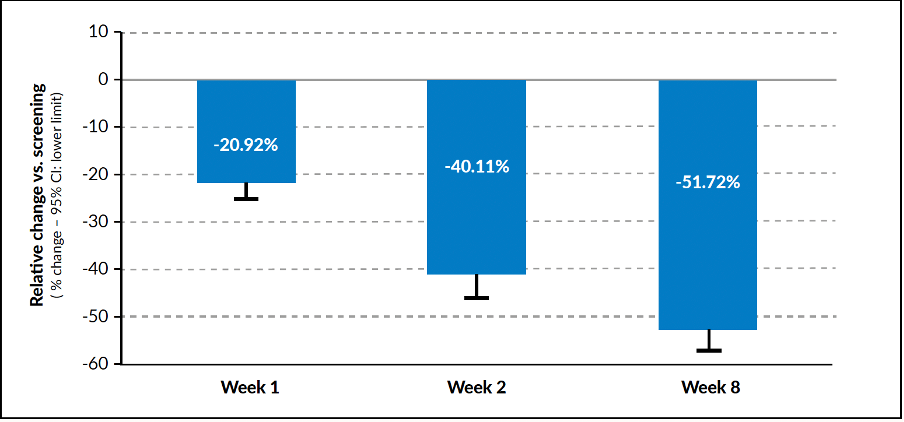
A third study enrolled 100 patients with prolonged or chronic fatigue symptoms, treated with WS® 1375 in an open-label multicenter single-arm clinical trial, for 8 weeks. Treatment effects were measured by changes of stress symptoms, fatigue, quality of life, mood, concentration, and general health. Again, improvement of symptoms was observed after 1 week of treatment. Fatigue continued to decline further, with a statistically significant improvement in week 8. In the MFI-20 scale significant improvements were reported in all 5 subscales (p<0.0001). In the subscale “general fatigue” at week 8 there was the greatest change with a difference to baseline of 8.2 ± 4.1 points. The evaluation in the scales on physical fatigue, mental fatigue, reduced activity, and reduced motivation, revealed changes at the end of the study of 6.9 ± 4.4, 6.0 ± 3.9, 6.5 ± 4.3 and 3.3 ± 3.3, respectively (mean ± standard deviation). The most pronounced changes in all MFI-20 subscales were seen already within the first week of treatment, followed by a continuous improvement up to the final visit in week 8 (Figure 5). Further, significant improvements (p<0.0001), similar among the different scales, were seen in all numeric analogue scales (NAS) for chronic fatigue symptoms according to the Center of Disease Control (CDC), which includes 3 self-ratings on post-exertional malaise, impairment of concentration/memory, and nonrestorative sleep.31
_(2.png)
In summary, it was remarkable in the three studies reported above that the patients rated a clear improvement in the symptoms of fatigue and exhaustion after already 1 week. In the further course of treatment, the effect increased, so that - even after 12 weeks of application - there was no “saturation”.
Further studies conducted with Rhodiola rosea extract also indicate that there is a clinical effect on fatigue: A significant improvement of fatigue was seen after 4 weeks of treatment in a study with 60 patients suffering from burnout-related fatigue,32 a lowered mental fatigue (besides improved complex perceptive and cognitive cerebral functions) was observed in 56 young volunteers (physicians) with fatigue during night duty after 2 weeks of treatment,33 and finally a continuously and highly significant reduction in the intensity of complaints was seen in 330 patients with burnout and exhaustion syndrome after 8 weeks of treatment.34
Rhodiola rosea extracts have been shown to be very well tolerated in all clinical studies and in post-marketing surveillance. The published literature does not give any reasons for concerns in respect to tolerability and safety. This is also reflected in the current Committee on Herbal Medicinal Products (HMPC) monograph on extracts from Rhodiola rosea roots and rhizomes which states that there are no known side-effects and no reported interactions. The HMPC of the European Medicines Agency’s (EMA) is responsible for compiling and assessing scientific data on herbal substances, preparations and combinations, to support the harmonization of the European market.35
Clinical trial data on WS® 1375 specifically in patients with post-COVID-19 symptoms are not yet available. Considering the study results reported above regarding the symptom fatigue, an effect on this characteristic main symptom of post-COVID-19 seems likely. This is also supported by the pharmacological mechanisms of action of Rhodiola rosea extracts known so far.
Summary and Conclusions
Rhodiola rosea extract WS® 1375 has a promising pharmacological and therapeutic profile for the treatment of fatigue and physical exhaustion associated with post-COVID-19 conditions. This is evident from clinical studies demonstrating significant improvement in the symptoms of fatigue and exhaustion in patients with various underlying conditions. Therefore, further studies with Rhodiola extracts of high quality such as in registered medicinal products with highest standards of quality control and quality assurance are warranted.
Corresponding Author
Siegfried Kasper MD
Professor Emeritus
Medical University of Vienna
Center for Brain Research
Department of Molecular Neuroscience
Spitalgasse 4, 1090 Vienna, Austria
Email: siegfried.kasper@meduniwien.ac.at
Conflict of Interest (COI)
TW: has received honoraria from Schwabe for writing manuscripts over the last years; DE: Androlabs, Bayer, Besins and Schwabe have paid honoraria and/or travel expenses and/or accommodation over the last three years; SK: has received grants/research support, consulting fees and/or honoraria within the last 3 years; grant/research support from Lundbeck; he has served as a consultant or on advisory boards Celegne, IQVIA, Janssen, Lundbeck, Mundipharma, Recordati, Takeda and Schwabe; and he has served on speakers bureaus for Angelini, Aspen Farmaceutica S.A., Janssen, Krka Pharma, Lundbeck, Medichem Pharmaceuticals Inc., Neuraxpharma, OM Pharma, Pierre Fabre, Sanofi, Servier, Schwabe, Sun Pharma.
Author Contributions
All authors participated in the conception, review of data and writing the review.
Funding
None.
Acknowledgments
Not applicable.