Introduction
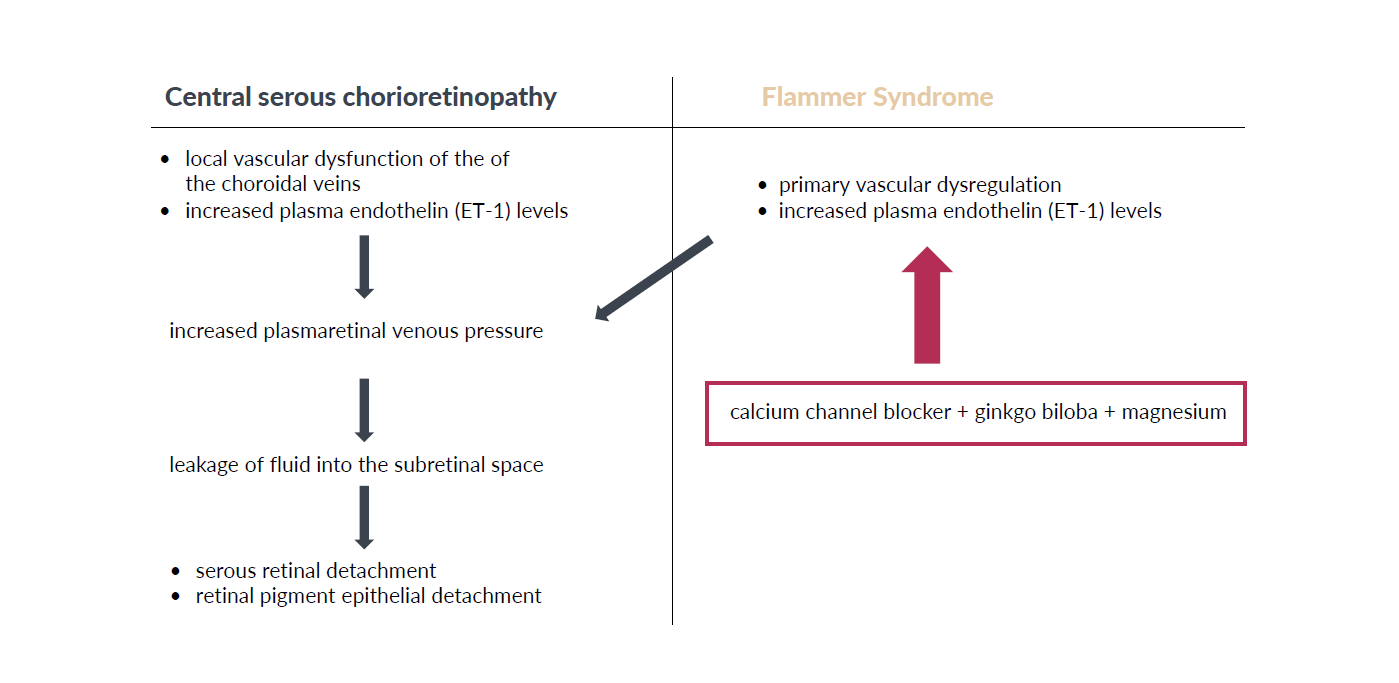
Patients with central serous chorioretinopathy (CSCR) develop serous retinal detachment and/ or retinal pigment epithelial detachment, particularly in the area of the macula, due to leakage of fluid through the retinal pigment epithelium into the subretinal space.1,2 Although the pathogenesis of this disease remains unknown, previous reports suggest an association of CSCR with the vascular dysregulation in the context of the Flammer Syndrome (FS) (Figure 1).3,4 FS is a benign and prevalent condition describing the phenotype of people who are generally healthy but have an altered reaction of blood vessels to stimuli such as cold or emotional stress.5,6 Similar to people with FS, who suffer from a primary vascular dysregulation,7,8 CSCR patients display a local vascular dysfunction of the of the choroidal veins.3 In both FS and in the acute phase of CSCR, plasma endothelin (ET-1) levels are increased.9,10 As a result, retinal venous pressure measured by means of ophthalmodynamometry is increased in FS patients.9,10
_and_flamme.png)
Case presentation
Clinical findings
A 57-year old woman presented with blurring of vision, cloudiness, and a dark spot on her right eye for a week. She has not been using any systemic or local corticosteroid medication but stated that she had suffered from emotional stress. Vascular anamnesis indicated that the patient suffered from FS: her hands and feet were frequently cold even during summer, she had low blood pressure, reduced feeling of thirst (she had to remind herself to drink enough fluid), and she suffered from migraines and at times from tinnitus. Her best corrected visual acuity was 0.8 in the right eye and 1.0 in the left eye. Anterior segment and intraocular pressure of 13 mm Hg (right eye) and 16 mm Hg (left eye) was normal. Retinal venous pressure was increased in both eyes to 23 mm Hg in the right eye and 25 mm Hg in the left eye (lack of a spontaneous retinal vein pulsation). Posterior segment examination of her right eye showed a serous retinal detachment. There were no signs of intraocular inflammation in either eye. The left eye showed normal posterior segment findings.
Treatment
Treatment aimed at the improvement of the vascular dysregulation in the context of FS. The patient received a low dosed calcium channel blocker (4 drops Nifedipine in a liter of water daily, ginkgo biloba (120 mg daily) and magnesium (12 mmol daily). At her four-months return visit, the best corrected visual acuity measured 20/20 in both eyes, retinal venous pressure values had basically normalized to 18 mm Hg in the right eye and 17 mm Hg in the left eye (IOP right eye: 14 mm Hg, IOP left eye: 12 mm Hg), and the posterior segment showed a resolution of the subretinal fluid.
Discussion
CSCR is characterized by an accumulation of subretinal fluid in the macula caused by abnormalities of the choroidal circulation.2 Although the disease generally affects the male population in their third and fourth decades,11 females may be affected as well. While the cause of CSCR remains unknown, several risk factors have been reported. In particular, the use of glucocorticoids12 and stressful events associated with higher endogenous corticosteroid levels have been correlated to the development of CSCR. Type A personality has also been reported to be associated with CSCR,13 along with other potential risk factors including us of tobacco, alcohol, sympathomimetic medication or psychotropic medication and autoimmune disorders.14
Abnormalities in the choroidal circulation play an important role in the pathogenesis of CSCR. Choroidal blood flow changes can be induced through enhanced oxidative stress, inflammatory cells and nitric oxide.7 The hyperpermeable choroidal vessels increase tissue hydrostatic pressure, leading to the breakdown of the blood retinal barrier.15 This in turn promotes pigment epithelial detachment and subretinal fluid accumulation. Back in 1996, when ocular blood flow measurements were performed in CSCR patients, C Prünte and J Flammer found that the patients had a delayed arterial filling followed by capillary and venous congestion.2 These observations support an involvement of primary vascular dysregulation in the context of the FS in these patients.
In short, although the origins of CSCR are yet unknown and various therapeutic options may be useful for individual patients, in patients with confirmed FS, treatment of vascular dysregulation may prevent CSCR or mitigate the course of the disease. Knowledge about the association of CSCR with FS may thus be useful for general practitioners, who tend to see the patients first.
Take-home messages
-
Patients with FS may suffer from CSCR due to FS-associated vascular dysregulation.
-
Treatment of the FS-associated vascular dysregulation can attenuate or resolve CSCR.
Conflict of Interest
None
Author Contributions
MM took the lead in writing the manuscript, JG made substantial contributions to the design, acquisition of data and presentation, LF contributed to the final version of the manuscript, provided critical feed-back and inserted references.
Funding
None
Acknowledgment
None