Introduction
Nontuberculous mycobacteria (NTM) are occasionally detected in respiratory specimen, but assessing their clinical significance is often challenging. Depending on the species and clinical context, it is important to distinguish whether the detected NTM is likely a contaminant or indicative of an infection. For NTM pulmonary disease, microbiological, clinical, and radiological criteria have been defined in statements by the ATS/ERS1 to assess the indication for treatment. NTM infections are a common cause of (cervical) lymphadenopathy in pediatric patients, but there are only few reported cases in adults.2,3 The treatment of NTM infections is complex and typically requires therapy with multiple anti-infective agents (≥3) over at least 12 months.1
Case presentation
We report the case of a 58-year-old male patient who initially presented to an outpatient clinic for further diagnostic evaluation of newly detected mediastinal lymphadenopathy. Seven years earlier, bilateral granulomatous panuveitis had been diagnosed, however despite extensive evaluation, no underlying associated disease had been identified. In the context of the newly diagnosed thoracic lymphadenopathy, sarcoidosis was considered the primary differential diagnosis.
Patient information / Personal history
The patient reported mild chronic exertional dyspnea (mMRC 1), morning cough, arthralgia, intermittent fever, general weakness and fatigue. Initially, no other B-symptoms were reported, later the patient reported an approximate weight loss of 5%. He was a smoker, consuming one pack of cigarettes per day, with no identifiable occupational exposures. At the time of the initial presentation, no medications were being taken. The patient had been treated with adalimumab until six years ago. In the interim, recurrent courses of systemic glucocorticoids were prescribed to treat uveitis flare-ups.
Clinical examination
Clinical findings were unremarkable. BMI was 21 kg/m². He was afebrile. The respiratory rate was normal, and SpO2 on ambient air was 96%. Pulmonary auscultation was normal. There were no signs of arthritis or synovitis, no skin lesions, and no palpable lymphadenopathy.
Diagnostic assessment
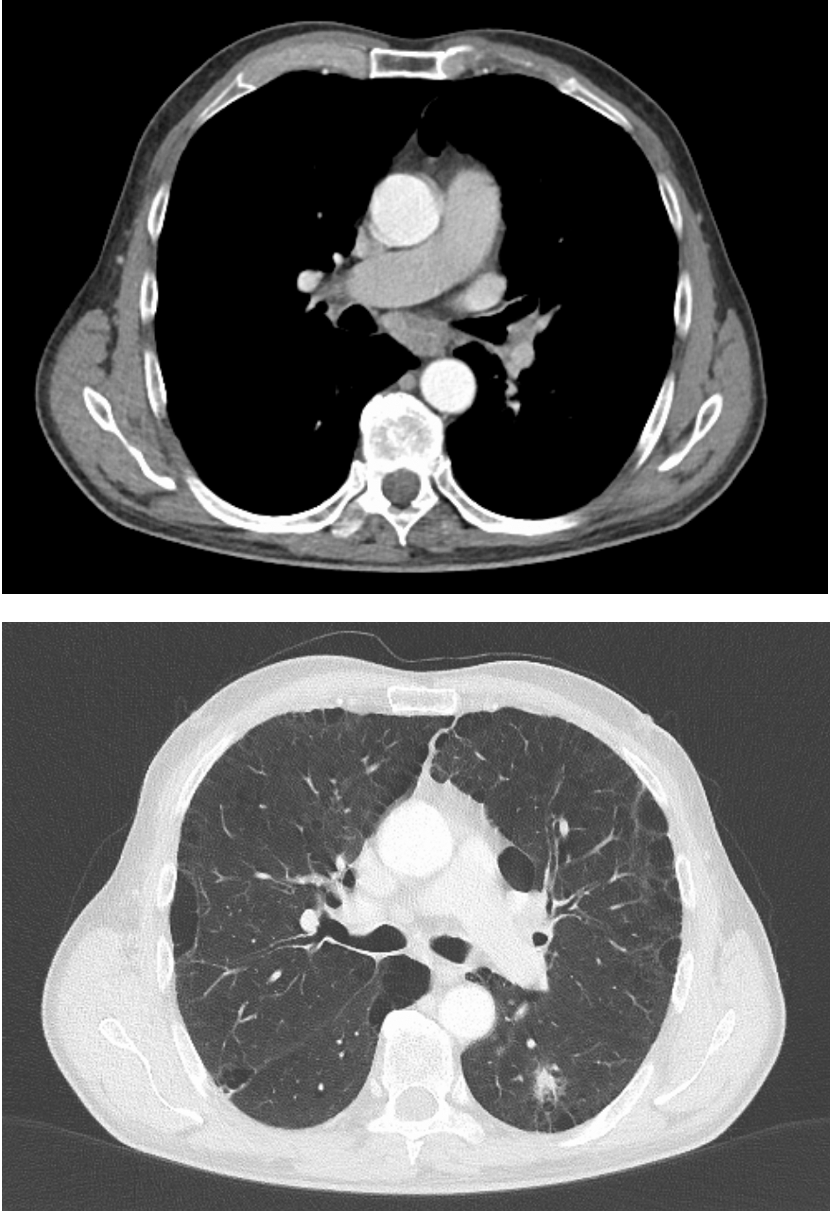
Computed tomography (CT) revealed enlarged mediastinal and hilar lymph nodes. Few isolated, nonspecific consolidations were present in the lung parenchyma, with no cavitary lesions or bronchiectasis. In addition, the CT demonstrated predominantly paraseptal bullous pulmonary emphysema, most likely related to smoking (Figure 1). Laboratory tests showed slightly elevated CRP. Blood counts indicated discrete normochromic normocytic anemia (Hb 130 g/l), along with recurrent mild leukopenia (around 3 × 10⁹/l) and neutropenia (min. 1.4 × 10⁹/l). Further tests revealed elevated soluble IL-2 receptor levels, a marker of T-cell activity usually correlating with disease activity in granulomatous disease, though not considered a diagnostic test for sarcoidosis.4 Serum calcium and ACE levels were normal, and the HIV screening test was negative.
_scan_of_the_thorax_(month_0).png)
Prior to admission to our clinic, bronchoscopy with endobronchial ultrasound (EBUS) had been performed. Bronchoalveolar lavage (BAL) revealed a representative sample with lymphocytosis (19.3%). Neither granuloma nor malignancy was observed in the mediastinal lymph node or in the transbronchial biopsy. Microbiology, including mycobacterial culture, was negative. Sarcoidosis could neither be ruled out nor confirmed based on these findings.
Lung function tests showed normal lung volumes but detected moderate CO diffusion impairment, in line with the pulmonary emphysema.
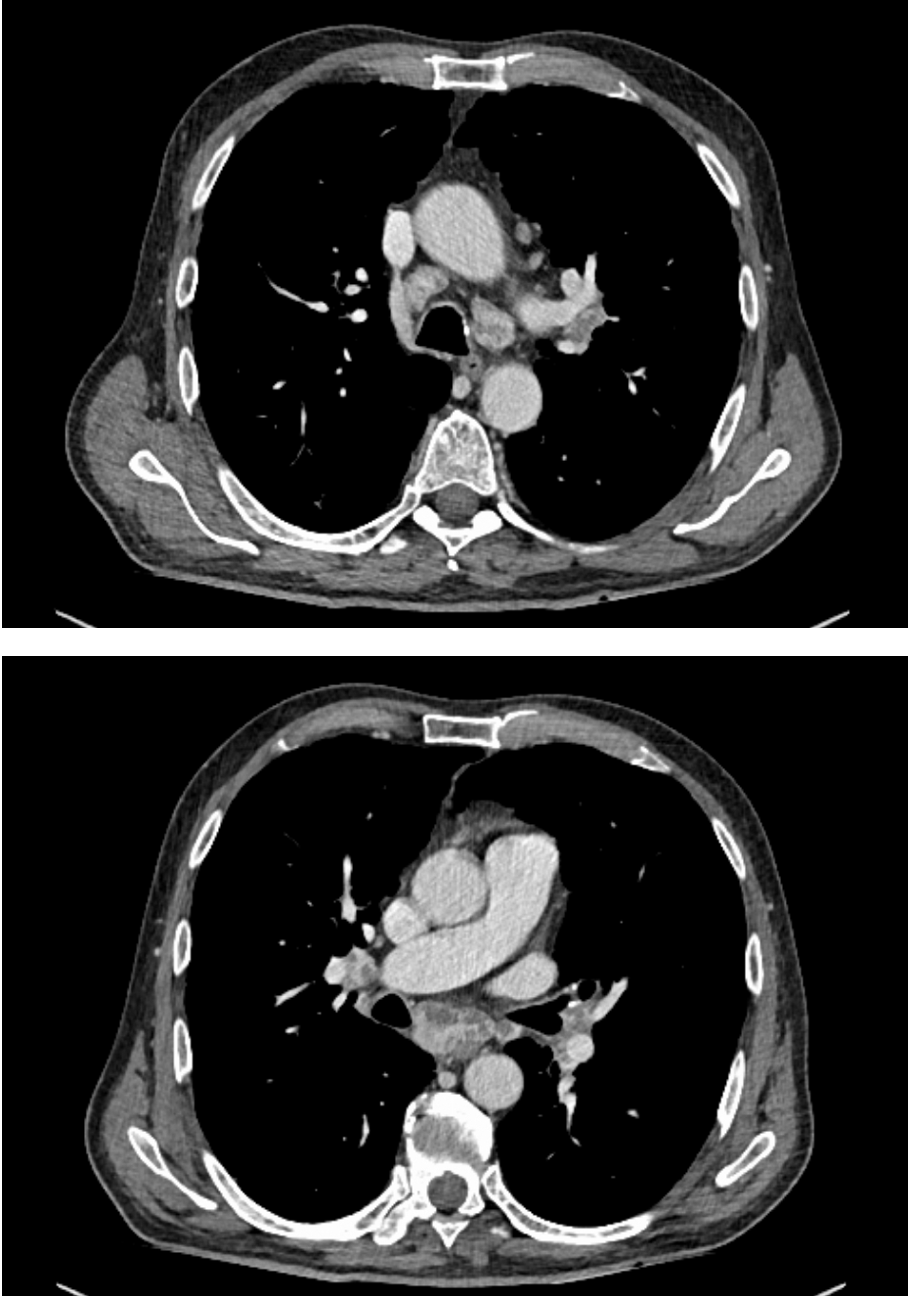
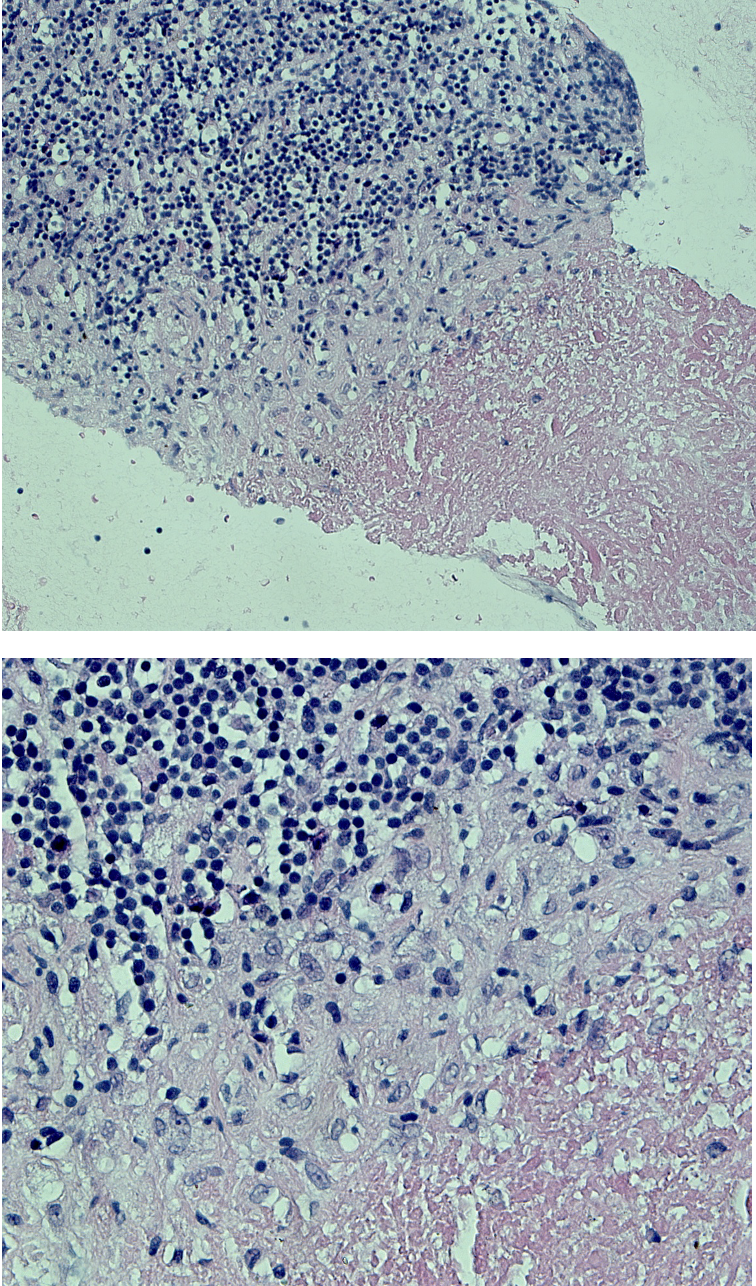
A follow-up CT scan six months later showed slight enlargement of the lymph nodes, now appearing distinctly inhomogeneous (Figure 2). The previously described consolidations in the lung parenchyma were no longer detectable, though a known solid pulmonary nodule persisted. A second bronchoscopy was scheduled. The lymph node biopsy revealed focal necrotic and granulomatous inflammation (Figure 3). Mycobacterium avium (M. avium) was detected in the lymph node sample by culture, direct microscopy revealed no acid-fast bacilli. Mycobacterial culture from the bronchial aspirate was negative. Polymerase chain reaction (PCR) testing for mycobacteria genus DNA from bronchial aspirate was negative. BAL was not repeated as there were no lesions in the lung parenchyma suggestive of NTM disease. Moreover, mycobacterial blood culture turned out negative.
_scan_of_the_thorax_(month_6).png)

In the meantime, repeated courses of systemic glucocorticoids were prescribed due to intermittent fever and musculoskeletal complaints with arthralgia. The symptoms responded well to steroids. Rheumatological evaluations were carried out, but no diagnosis was made. In particular, spondylarthropathy as a potential association with recurrent panuveitis was not confirmed nor was there evidence for arthropathy associated with sarcoidosis.
Therapeutic intervention
According to ATS/ERS guidelines,1 the detection of M. avium in a single tissue sample is considered sufficient for diagnosis, with no need for verification from a second sample as opposed to sputum samples, for example. However, the guidelines refer to lung biopsy samples, not lymph node samples. Furthermore, pulmonary or systemic symptoms are required, as well as CT evidence of nodular or cavitary lesions or multifocal bronchiectasis with multiple small nodules. All criteria must be met in order to diagnose NTM lung disease. We are not aware of any criteria or management recommendations for isolated mediastinal lymphadenopathy due to NTM in adults, or treatment recommendations for extrapulmonary NTM disease in general.
In this case, microbiological criteria were met. However, continued smoking and emphysema could also partially explain the reported symptoms. The few pulmonary consolidations as detected in the initial CT scan cannot definitively be attributed to NTM infection.
Following an interdisciplinary discussion and consultation with the patient, the decision was made to initiate antibiotic therapy. This decision was also based on the assumption that ongoing immunosuppressive therapy would be required in the future, because although no definite diagnosis had been made yet, we still suspected an underlying condition due to recurrent symptoms including intermittent fever leading to rheumatological examinations as discussed above.
According to resistance test results (Table 1) and ATS/ERS recommendations, an oral treatment with azithromycin, rifampicin, and ethambutol three times per week was initiated. Unfortunately, two weeks after the start of therapy, a severe drug rash developed, requiring treatment discontinuation. The patient was evaluated by dermatology specialists, however, he refused allergy tests.
Given the occurrence of relevant adverse effects, along with no lung parenchymal changes regarding the NTM infection and few respiratory symptoms, a watchful approach was decided.
Follow-up
A follow-up CT scan 2.5 months later of the neck, thorax, and abdomen showed unchanged mediastinal and bilateral hilar lymphadenopathy with small calcifications and hypodense areas. No additional lymphadenopathy was present within the examined volume, and no new or progressive lung parenchymal changes were observed. Bronchoscopy confirmed the previous findings, once again revealing centrally necrotizing granulomas in the lymph nodes. Cultures from the lymph node sample were positive for M. avium.
Outcome
The blood count abnormalities described above were initially variable, possibly reactive due to chronic inflammation. Due to blood count changes, including persistent monocytopenia (0.0–0.1 G/l), intermittent lymphocytopenia, progressive neutropenia and anemia, a hematologic-oncologic workup was performed, leading to the diagnosis of BRAF V600E mutated hairy cell leukemia (HCL). First-line therapy for HCL consists of purine analogues. However, these agents cause profound T-cell depletion, consequently leading to severe immunosuppression. Therefore, therapy with the BRAF inhibitor vemurafenib was decided upon and initiated. In the following days, the patient experienced rapid clinical deterioration with the onset of severe distributive shock along with respiratory and renal insufficiency, acute cholestatic hepatitis, and possible hemophagocytic lymphohistiocytosis. Empiric anti-infective therapy with Meropenem and Voriconazole for septic shock was initiated. Diagnostic workup in the ICU revealed M. avium in blood cultures and bronchial aspirates, indicating disseminated M. avium infection in the now severely immunocompromised patient. NTM treatment with azithromycin, amikacin and clofazimine was started. There were no side effects clearly attributable to the newly added medication. However, there was no improvement and after several significant complications, intensive care measures were discontinued, and the patient passed away within a day, 13 days after NTM treatment was initiated.
Discussion / Literature review
Nontuberculous mycobacteria (NTM) can cause both asymptomatic infections and symptomatic disease in humans.5 Epidemiological data show an increase in the prevalence of NTM infections. In North America and East Asia, M. avium complex (MAC) is predominant, whereas M. kansasii, M. xenopi, and M. malmoense are more common in Europe. NTM lung disease is more common in patients with structural lung disease, including COPD and emphysema, as seen in our case. Steroid use and anti-TNF agents are recognized risk factors for NTM disease.6
Disseminated NTM disease is associated with immunodeficiency, either acquired (including iatrogenic) or genetic.7 Hairy cell leukemia, as described in this case, is a known risk factor for disseminated NTM disease.8
Data on lymph node samples in adults is limited. Data from Oregon over 2 years shows a total of 21 cases (prevalence 0.3/100,000) of MAC lymphadenitis (without specifying lymph node region), compared to 344 cases of MAC pulmonary disease (4.7/100,000).2 Data from France lists five cases of lymphadenitis (without specifying location) over 3 years from 304 MAC isolates.9 Most case reports of MAC lymphadenitis in adults address cervical lymphadenitis.10 NTM lymphadenitis is much more common in children, where NTM infection is the most common cause of lymphadenitis.3
There is limited data on mediastinal lymphadenopathy in NTM disease, especially as EBUS bronchoscopy has become a widely used diagnostic tool.11 EBUS-TBNA is an established diagnostic tool for mediastinal tuberculous lymphadenitis.12
The challenge remains in determining when and whom to treat, as we are not aware of any guidelines or recommendations for NTM mediastinal lymphadenopathy. We had to refer to guidelines addressing NTM pulmonary disease.
The observed hematologic abnormalities, including monocytopenia, may retrospectively be interpreted as early indicators of an underlying hematologic malignancy. Given the progressive deterioration of blood counts over time, alongside the dissemination of the NTM infection, we consider hairy cell leukemia (HCL) to be the primary predisposing factor for the progression of NTM disease. We also assume that the patient’s symptoms, especially B-symptoms, were caused by HCL. Treatment with vemurafenib was initiated only a few days prior to clinical deterioration. An earlier diagnosis of HCL might have prevented or at least delayed the progression of the NTM infection.
Conclusions / Take-home messages
We described a rare case of mediastinal lymphadenopathy due to M. avium infection in an adult patient.
The course of this case suggests that hairy cell leukemia, diagnosed one year after NTM lymphadenitis, might have been present for a longer period and could have been an additional risk factor for the development of mediastinal lymphadenitis due to MAC and, particularly, for disseminated NTM disease. Other risk factors for NTM disease in this patient included recurrent systemic glucocorticoid use, previous TNF-inhibitor therapy, and pulmonary emphysema.
Infection with nontuberculous mycobacteria should be considered when histopathological samples show caseating granulomas without evidence of tuberculosis. It is important to order specific laboratory tests if NTM infection is considered.13 We suggest actively ruling out underlying conditions causing immunodeficiency, particularly in patients with confirmed NTM disease and no known risk factors.
Acknowledgements
We thank PD Dr Gunar Günther and Dr Matthias Hoffmann for their expert input and insightful discussions regarding this case.
Consent to participate
The legal representative of the patient gave their informed consent on publishing the patient’s medical data to this case.
Availability of data and materials
All patient data that support this case report are included in anonymized form in the published article.
Conflict of interest
The author(s) has (have) declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript. CW drafted the manuscript. RF and CR revised the manuscript. MS carried out the histological analysis and provided the images.