Introduction
Septic shock represents the most severe progression of sepsis and remains a leading cause of mortality in intensive care units, with death rates reaching up to 40%.1–4 The condition is characterized by profound circulatory, cellular and metabolic dysfunction, including persistent hypotension, tissue hypoperfusion and elevated lactate levels resulting from a dysregulated host response to infection.1,4,5 Hemodynamic management of septic shock and other vasodilatory states relies on adequate fluid resuscitation and vasopressor therapy when volume expansion alone fails to restore blood pressure and tissue perfusion. Vasopressors are categorized into catecholamines (e.g. norepinephrine, epinephrine) and non-catechol-aminergic agents (e.g. vasopressin, angiotensin II).6 The latter, also referred to as pure vasoconstrictors, act exclusively on blood vessels without direct cardiac effects, reducing the risk of cardiac toxicity.7
In contrast, catecholamines also increase cardiac output and heart rate by activating β1 receptors. At higher doses, catecholamine use in septic shock is associated with serious adverse cardiac events such as atrial fibrillation and ventricular arrhythmias.8–10 Still, norepinephrine remains the first-line vasopressor due to its consistent vasoconstrictive effects, minimal impact on heart rate and mild β1 activity, which may help support cardiac output.6 Excessive norepinephrine exposure has long been suspected to contribute to adverse outcomes in septic shock.11 While vasopressor dose is undoubtedly linked to illness severity,12 accumulating evidence suggests that high-dose norepinephrine may also be independently associated with harm.13,14 Mortality may increase dramatically at very high doses, with rates approaching 90% in patients receiving ≥1 μg/kg/min.11 This has prompted interest in adjunctive therapies that not only to reduce catecholamine requirements,13,14 but also to restore vascular tone through non-adrenergic mechanisms while addressing the phenomenon called relative vasopressin deficiency identified in septic shock.15 Importantly, vasopressin has been shown to be non-inferior to norepinephrine in terms of survival when used as first-line therapy, further supporting its role as a rational second-line agent.16 This underscores the need for an adjunctive, catecholamine-sparing option such as vasopressin in patients with catecholamine-refractory septic shock.
SSC Guidelines for the management of sepsis and septic shock – Need for additional guidance
The 2021 International Guidelines for Management of Sepsis and Septic Shock of the Surviving Sepsis Campaign (SSC) recommend norepinephrine as the first-line vasopressor over dopamine, vasopressin, epinephrine, selepressin and angiotensin II in septic shock.17 Vasopressin received a weak recommendation as a second-line agent when MAP remains inadequate despite norepinephrine doses between 0.25 and 0.5 μg/kg/min after adequate fluid resuscitation, rather than further increasing norepinephrine. In contrast, terlipressin – a synthetic vasopressin analogue with higher V1a receptor selectivity and longer half-life – is not recommended.17 While the SSC guidelines acknowledge the role of vasopressin, they do not address key practical questions regarding dosing, weaning strategies, or the preferred order of vasopressor discontinuation, leaving clinicians to rely on local protocols or expert consensus.17 This recommendation to deliberate vasopressin raises uncertainties about when to define refractoriness, when to introduce a second agent and which agent to choose. Various publications have sought to address these gaps with pragmatic strategies.18–22
Vasopressin (argipressin, Empressin®) is currently the only non-sympathomimetic vasoconstrictor approved in Switzerland for the treatment of catecholamine-refractory hypotension in adults with septic shock, defined as a failure to stabilize MAP to 65–75 mmHg despite adequate volume resuscitation and catecholamine therapy.23 There is no unified definition of catecholamine-refractory septic shock in the scientific literature. Reported norepinephrine thresholds vary widely, from 0.2–4 μg/kg/min, with most studies considering doses ≥0.5–1 μg/kg/min as indicative of refractoriness.24 Clinically, this state is typically defined by persistent circulatory failure despite adequate fluid resuscitation and high-dose norepinephrine therapy, as described in multiple observational and interventional studies.11,24,25
Methodology
The 2nd Swiss Vasopressin Consensus Report was developed following a face-to-face expert meeting held in December 2024, complemented by a structured electronic feedback process.
Recommendations were formulated by critically weighing the risks and benefits of each intervention against the background of current scientific and clinical evidence. Levels of Evidence and Classes of Recommendation were assigned based on grading principles aligned with the standards of the European Society of Cardiology (ESC)26 and consistent with widely accepted international practices, as outlined in Table 1 and Table 2.27,28
A preliminary consensus on each recommendation was achieved through structured group discussion during an in-person meeting, followed by refinement in a subsequent conference call. Thereafter, an anonymous electronic survey was conducted, using interactive forms to enable standardized voting on the proposed Class of Recommendation and Level of Evidence. If the initial vote did not reach at least 75% affirmative responses (i.e. the generally accepted threshold for consensus26,27), a second anonymous voting round was initiated to strengthen agreement among participating experts. A response rate of ≥87.5% was achieved in both electronic rounds. Remaining differences in the strength of recommendation were resolved through a third round of open, asynchronous discussion via email among all panel members.
Definition of vasoplegic syndrome
Circulatory failure (shock) is a common and life-threatening condition in critically ill patients. It typically results from either reduced cardiac output – as seen in cardiogenic, hypovolemic, or obstructive shock – or from decreased systemic vascular resistance, known as vasoplegic shock. The latter is characterized by peripheral vasodilation, microcirculatory dysfunction and often increased vascular permeability, contributing to relative hypovolemia.29 These mechanisms occur in various clinical settings, including septic shock, anaphylactic shock and systemic inflammatory states such as after major surgery with prolonged cardiopulmonary bypass, major surgery, burns, trauma, or hemorrhage.30,31 Vasoplegia reflects a loss of vascular smooth muscle responsiveness to endogenous vasoconstrictors and typically necessitates the use of exogenous vasopressors.
Septic shock, a specific form of vasoplegic shock, is defined by the Sepsis-3 criteria as persistent hypotension as a consequence of a dysregulated host response to infection, requiring vasopressor therapy to maintain MAP ≥65 mmHg and serum lactate levels >2 mmol/L despite adequate fluid resuscitation.5 However, hemodynamic instability in septic shock is often multifactorial and may involve varying degrees of cardiac dysfunction as well as relative and absolute hypovolemia.4,29
Vasopressin in Septic Shock
Physiology
Vasopressin, also known as arginine vasopressin, argipressin, or antidiuretic hormone (ADH), is a non-catecholamine vasopressor and antidiuretic hormone synthesized in the hypothalamus and released by the posterior pituitary gland in response to hypotension, hypovolemia and increased plasma osmolarity.32,33 Hypovolemia and hypotension activate atrial volume receptors and carotid baroreceptors, stimulating vasopressin secretion. Vasopressin has a short plasma half-life of 5–15 minutes, with clearance primarily dependent on renal and hepatic vasopressinases.34 It exerts its vasopressor effect mainly through V1 receptor stimulation on vascular smooth muscle cells, increasing systemic vascular resistance and improving arterial and coronary perfusion pressure without affecting pulmonary vascular resistance. Other effects of V1 stimulation include endothelial release of nitric oxide (NO).33,35 This NO release may locally counteract V1-mediated vasoconstriction by promoting cGMP-mediated smooth muscle relaxation, particularly in vascular compartments with high endothelial receptor sensitivity.33,35 V2 receptor activation promotes water reabsorption in the renal collecting ducts, while V1b (V3) receptor activation in the pituitary increases adrenocorticotropic hormone (ACTH) release and raises serum cortisol levels.33
Unlike catecholamines, vasopressin does not act on α- or β₁-adrenergic receptors and thus induces vasoconstriction via a catecholamine-independent pathway.33 This makes vasopressin particularly valuable in catecholamine-refractory shock, where adrenergic receptor desensitization occurs. In addition, vasopressin has no direct inotropic effect and does not provoke arrhythmias.6,36,37 By reducing catecholamine requirements, vasopressin also minimizes β₁ receptor stimulation and lowers myocardial oxygen demand.38,39
Key Rationales for the Use of Vasopressin in Septic Shock
One of the key physiological rationales for using exogenous vasopressin in septic shock is the phenomenon of relative vasopressin deficiency. During the early phase of septic shock, vasopressin levels initially rise but then decline sharply within 72 hours despite ongoing hypotension and may remain pathologically low for up to seven days.16,40 This depletion of neurohypophyseal stores and impaired vasopressin synthesis contributes to persistent hypotension, as evidenced by the marked pressor response to exogenous vasopressin administration.15 In contrast to the adrenoceptor desensitization caused by high circulating catecholamine levels, vasopressin receptor sensitivity remains unaffected.41
In addition to this pathophysiological rationale, early vasopressin initiation may offer clinical benefit by preventing escalation to high-dose norepinephrine therapy. In a retrospective cohort of 1,610 patients with septic shock, Sacha et al. found that hospital mortality increased by 20.7% for each 0.15 μg/kg/min increase in norepinephrine-equivalent dose at the time of vasopressin initiation.13 Outcomes were most favorable when vasopressin was initiated before norepinephrine exceeded approximately 0.15 μg/kg/min (approx. 10 μg/min in a 70 kg patient) and when lactate levels remained below 2.3 mmol/L. These findings align with earlier work by Dünser et al., who demonstrated that vasopressor load itself – independent of disease severity – was associated with increased mortality.14 Together, these data support the rationale for early vasopressin use to limit catecholamine burden and avoid progression to vasopressor-refractory shock.11
Vasopressin in septic shock: Major clinical studies
Observational studies/Cohort studies
A multicenter observational study by White et al. (2024) investigated the impact of vasopressin initiation timing on hospital mortality among 2,747 septic shock patients across twelve ICUs in Australia.42 Early vasopressin initiation (within six hours of starting vasopressor therapy) occurred in 67% of patients and was independently associated with lower hospital mortality (35% vs 40%; adjusted odds ratio [aOR]: 0.69 [95% CI: 0.57–0.83]).use was linked to reduced norepinephrine requirements, improved arterial pH, lower lactate concentrations and less tachycardia. These findings suggest that early adjunctive vasopressin initiation may improve outcomes in septic shock and warrant further prospective investigation.42
A real-world cohort study based on MIMIC-III and MIMIC-IV database data retrospectively analyzed 1,817 septic shock patients.43 Patients were stratified according to norepinephrine-equivalent dose at vasopressin initiation: a low-dose group (<0.25 μg/kg/min) and a high-dose group (≥0.25 μg/kg/min). After propensity score matching, baseline illness severity (SOFA, SAPS II and LODS scores) was comparable between groups. Early vasopressin initiation in the low-dose group was associated with a significantly lower 28-day mortality (49.2% vs 59.4%; OR: 0.660; p<0.001), shorter norepinephrine exposure (p=0.014), less fluid accumulation (p=0.006) and improved renal function. While reduced fluid requirements may reflect earlier hemodynamic stabilization, these associations remained significant across multiple statistical models, suggesting a potential clinical benefit.43
Randomized clinical trials (RCTs)
The VASST trial was the first large, randomized study comparing vasopressin with norepinephrine in septic shock. It evaluated norepinephrine alone versus norepinephrine plus vasopressin (0.01–0.03 U/min) in 778 patients. The primary outcome, 28-day mortality, showed no significant difference between groups (35.4% vs 39.3%; p=0.26).16 However, a predefined subgroup analysis revealed that patients with less severe septic shock (i.e. lower norepinephrine requirements at randomization, 5–14 μg/min) experienced a nearly 10% absolute reduction in 28-day mortality with vasopressin (26.5% vs 35.7%; p=0.05), suggesting a possible benefit of earlier vasopressin use. A key limitation of the VASST trial was the relatively high baseline MAP (approximately 72 mmHg), indicating that many patients were not truly catecholamine-refractory, potentially diluting any treatment effect. Notably, the study was also underpowered due to a lower-than-expected mortality rate (39.3% observed vs 60% projected), potentially limiting its ability to detect a survival benefit.16
A post-hoc analysis of VASST focused on renal outcomes.44 In patients “at risk” for acute kidney injury (RIFLE-R), vasopressin was associated with a significantly lower rate of kidney disease progression (20.8% vs 39.6%; p=0.03) and a reduced need for renal replacement therapy (17.0% vs 37.7%; p=0.02) compared to norepinephrine. These effects were not observed in patients with established or advanced renal injury (RIFLE-I or -F). A subgroup analysis further suggested that mortality was lower when vasopressin was initiated at norepinephrine-equivalent doses of 0.15 μg/kg/min or at lactate levels below 2.3 mmol/L, compared to delayed initiation at higher doses or higher lactate concentrations.44
The VANISH trial compared early vasopressin as the first-line vasopressor with norepinephrine in septic shock but found no significant difference in kidney failure-free days over 28 days (57.0% vs 59.2%; [95% CI: −13.0 to −8.5]).45 However, vasopressin was associated with a lower need for renal replacement therapy (25.4% vs 35.3%; [95% CI: −19.3 to −0.6]), despite no significant differences in creatinine levels or urine output. The 28-day mortality was comparable between norepinephrine and vasopressin (30.9% vs 27.5%; [95% CI: −5.4−12.3]). Although the study did not demonstrate a survival benefit, the 95% confidence interval (95% CI: −11−5) of the difference between groups had an upper limit favoring vasopressin, suggesting a potential clinical benefit and indicating the need for larger trials. The VANISH trial employed twice the vasopressin dose used in VASST (0.01–0.06 U/min), based on the hypothesis that higher dosing might confer a survival advantage not observed in VASST; however, no survival benefit was demonstrated.45
The VANCS II trial, a randomized, double-blind study in 250 cancer patients with septic shock, also found no mortality benefit for vasopressin over norepinephrine at 28 days (56.8% vs 52.8%; p=0.52) or 90 days (72.0% vs 75.2%; p=0.56). Secondary outcomes were comparable, but patients receiving vasopressin required more rescue norepinephrine, suggesting incomplete hemodynamic stabilization with vasopressin monotherapy.46
Systematic reviews and meta-analyses
A systematic review by Webb et al. (2020) included three randomized controlled trials and one retrospective cohort study, totaling 708 patients with vasoplegic shock.47 The findings were inconclusive and showed no clear superiority of vasopressin over alternative vasopressors. Potential benefits were observed regarding acute kidney injury, atrial arrhythmias and vasopressor duration. However, vasopressin did not reduce 30-day mortality or the incidence of ventricular arrhythmias. Interpretation was limited by mixed methodologies, small sample sizes and heterogeneous study populations.47
An individual patient data meta-analysis by Nagendran et al.48 included 1,453 patients with septic shock from VASST (n=779),16 VANISH (n=409),45 VANCS II (n=250)46 as well as from the Dünser et al. trial (n=15).49 Vasopressin did not reduce 28-day mortality (RR: 0.98 [95% CI: 0.86–1.12]) compared to other vasoactive agents. However, it was associated with a decreased need for renal replacement therapy (RRT) (RR: 0.86 [95% CI: 0.74–0.99]). This effect was not robust in sensitivity analyses, as the confidence intervals included both benefit and no effect. No significant interactions were observed in predefined subgroups, leaving the overall impact of vasopressin on renal function uncertain.48 A systematic review and meta-analysis by Nedel et al. included 17 RCTs with 2,833 patients with distributive shock. Vasopressin and its analogs were associated with a reduced need for renal replacement therapy (OR: 0.59 [95% CI: 0.37–0.92]; p=0.02) and a lower incidence of acute kidney injury (OR: 0.58 [95% CI: 0.37–0.92]; p=0.02). Subgroup analyses suggested greater renal benefits in vasoplegic shock than in septic shock, with lower heterogeneity when stratified by shock type. However, the quality of evidence was rated low to moderate due to study heterogeneity (I²=49% for RRT; I²=63% for acute kidney injury incidence).50
A meta-analysis by Zhong et al. (2020) pooled data from 23 RCTs involving 4,380 patients with septic shock.51 Adding non-catecholamine vasopressors (vasopressin, pituitrin, terlipressin, selepressin, or angiotensin II) to norepinephrine therapy resulted in a modest reduction in 28-day mortality (RR=0.92 [p=0.02]). Subgroup analyses indicated a potential survival benefit in catecholamine-resistant refractory shock (RR: 0.84; p=0.048) but not in the general septic shock population. These benefits were offset by an increased risk of digital ischemia (RR: 2.43 [95% CI: 1.39–4.25]).51
A more recent meta-analysis by Kotani et al. (2024) included 51 RCTs across septic shock, cardiac surgery and non-cardiac surgery settings (n=5,715).52 Non-adrenergic vasopressors slightly reduced mortality in septic shock (RR=0.92 [p=0.03]) and were associated with reduced use of renal replacement therapy and a lower incidence of atrial fibrillation. However, no individual agent demonstrated a statistically significant survival benefit. The authors noted that heterogeneity in dosing strategies and patient populations limits generalizability.52
Adverse Effects
Due to its potent vasoconstrictive effect, vasopressin has raised concerns about potential ischemic complications. According to the Swiss SmPC of Empressin® (vasopressin, argipressin), the most frequent serious adverse effects include digital ischemia, mesenteric ischemia, acute myocardial ischemia and life-threatening arrhythmias, although their reported incidence is below 10%.23 Clinical trials found no evidence that these adverse events occurred more frequently with vasopressin than with norepinephrine, except for digital ischemia. In the VASST trial, serious adverse events were comparable between groups; however, digital ischemia and hyponatremia were more frequent with vasopressin, while cardiac arrests occurred more often with norepinephrine.16
In the VANCS trial, which compared vasopressin (0.01–0.06 U/min) to norepinephrine in vasoplegic shock after cardiac surgery, no significant differences were observed in the incidence of digital ischemia, mesenteric ischemia, hyponatremia, or myocardial infarction. Notably, atrial fibrillation occurred significantly less frequently in the vasopressin group (63.8% vs 82.1%; p=0.0004).53 Consistent with these findings, a separate meta-analysis by McIntyre et al., including 23 randomized clinical trials with 3,088 patients, found that vasopressin as add-on to catecholamines in distributive shock including septic shock and vasoplegia after cardiac surgery significantly reduced the risk of atrial fibrillation compared to catecholamines alone (RR: 0.77 [95% CI: 0.67–0.88]).54
Regarding ischemic complications, consistent signals for increased digital ischemia have been identified in both individual patient data and aggregate meta-analyses. In before-mentioned individual patient data meta-analysis by Nagendran et al.,48 including VASST (0.01–0.03 U/min),16 VANISH (up to 0.06 U/min),45 VANCS II (0.01–0.06 U/min),46 Dünser et al. (up to 0.066 U/min),49 vasopressin use was associated with a higher incidence of digital ischemia (absolute risk difference [ARD]: 1.7 [95% CI: 0.3–3.2]), whereas rates of mesenteric and coronary ischemia were comparable between groups.48 In a separate aggregate-data meta-analysis by Yao et al., which included vasopressin and its analogs (terlipressin, selepressin), vasopressin receptor agonists were associated with a significantly increased risk of digital ischemia compared to catecholamines alone (RR: 2.65 [95% CI: 1.26–5.56]; p<0.01). In contrast, the risk of acute mesenteric ischemia remained similar between groups (RR: 0.99 [95% CI: 0.60–1.63]; p=0.96).55
High vasopressin doses with intense V1-mediated vasoconstriction in the splanchnic circulation can cause acute mesenteric ischemia. Although rare, the latter remains a serious complication.56 Experimental studies in fluid-resuscitated porcine models of septic shock have demonstrated that vasopressin at doses of 0.06 U/kg/h causes marked reductions in portal vein flow (-58%), pancreatic microcirculation (-45%) and jejunal mucosal flow (-27%), despite improvements in systemic arterial pressure.57,58 These effects were particularly pronounced under conditions of impaired cardiac output, suggesting that vasopressin-induced vasoconstriction may critically impair regional oxygen delivery even after fluid resuscitation. This mismatch between improved global perfusion and compromised regional microcirculation has been proposed as a mechanistic contributor to non-occlusive acute mesenteric ischemia (NOMI).59 Ischemic skin lesions, another possible manifestation of impaired regional perfusion, have been observed in up to one-third of patients, with peripheral arterial disease and septic shock identified as independent risk factors in multivariate analysis.60
This mechanistic evidence is supported by clinical observations. A WHO pharmacovigilance analysis of over 24 million reports identified a significant signal for acute mesenteric ischemia (AMI) specifically associated with vasopressin (Reporting Odds Ratio [ROR]: 30.15 [95% CI: 17.76–51.20]), comparable to norepinephrine (ROR: 28.70), whereas no signal was detected for selepressin.59 Additionally, two retrospective clinical studies evaluating vasopressin at doses up to 0.06 U/min reported improved hemodynamic control compared to the 0.03 U/min used in VASST but also a higher incidence of adverse effects, including mesenteric ischemia, cholestasis and thrombocytopenia.61,62
Taken together, these findings suggest that vasopressin does not increase the overall incidence of serious adverse events compared to norepinephrine. However, ischemic complications – particularly digital ischemia – remain a relevant concern. This association was consistently observed in randomized controlled trials.48,55 In contrast, signals for acute mesenteric ischemia have been reported primarily in pharmacovigilance databases21 and retrospective analyses,61,62 while no significant difference was found in RCTs.48,55 Vasopressin dose escalation should therefore be approached with caution, especially at higher doses and in patients with impaired peripheral or splanchnic perfusion.
Treatment Initiation and dose escalation
Vasopressin Initiation
The 2021 SSC Guidelines recommend initiating vasopressin when the norepinephrine dose reaches 0.25–0.5 μg/kg/min, rather than delaying until a catecholamine-refractory shock develops.17
In contrast, a recent target trial emulation by White et al. (2025)63 provided strong evidence in favor of earlier vasopressin initiation. Among 3,105 patients with septic shock, vasopressin administration within the first 6 hours of vasopressor therapy and at norepinephrine-equivalent doses <0.25 μg/kg/min was associated with significantly lower 30-day ICU mortality. The mortality benefit was most evident in patients with elevated lactate levels (>4 mmol/L) and in those requiring mechanical ventilation. These findings challenge the broader initiation range suggested by the SSC 2021 guidelines and support the consideration of earlier intervention in high-risk populations.63
In the retrospective, propensity-score matched VISPSS cohort, vasopressin initiation at norepinephrine-equivalent doses <0.25 µg/kg/min was associated with lower 72-hour fluid balance compared with delayed initiation (≥0.25 µg/kg/min), without differences in vasopressor duration or mortality. Earlier initiation (≤4 hours) was independently associated with shorter time to shock resolution.64
A recent simulation study by Kalimouttou et al. applied reinforcement learning to large ICU datasets to evaluate vasopressin timing in septic shock.65 The model generated treatment decisions based on norepinephrine dose, shock duration, lactate levels and SOFA score and consistently favored earlier and more frequent vasopressin use than observed in routine practice. Although no fixed initiation threshold was defined, the strategy was associated with lower predicted mortality and supports the rationale for earlier intervention.65
These findings are complemented by a prospective multicenter registry study by Melchers et al. (2025) from the van Zanten team, which evaluated vasopressin response in 200 patients with septic shock across 11 ICUs. A norepinephrine dose ≥0.30 μg/kg/min at initiation was significantly associated with a positive hemodynamic response, while hyperlactatemia, obesity and low pH predicted reduced responsiveness. The results suggest that patient-specific factors and vasopressor burden may help identify individuals most likely to benefit from vasopressin therapy.66
It should be noted that norepinephrine requirements of approximately 0.2 μg/kg/min do not necessarily indicate a clinically relevant vasoplegic syndrome, particularly in deeply sedated patients. A recent cohort analysis comparing propofol and midazolam in septic ICU patients found that both sedatives were associated with increases in norepinephrine doses in the range of 0.1–0.2 μg/kg/min, suggesting that vasopressor needs may be significantly influenced by the depth and type of sedation.67 In other words, a moderate norepinephrine dose in a deeply sedated patient does not necessarily indicate worsening shock – it could be the effect of the sedation on vascular tone.
Vasopressin dosing and dose escalation
Clinical studies in septic shock (VASST, VANISH, VISPSS) and vasoplegic shock after cardiac surgery (VANCS) consistently recommend vasopressin dosing between 0.01 and 0.03 U/min, with most patients effectively stabilized around 0.02–0.03 U/min.16,45,46,53
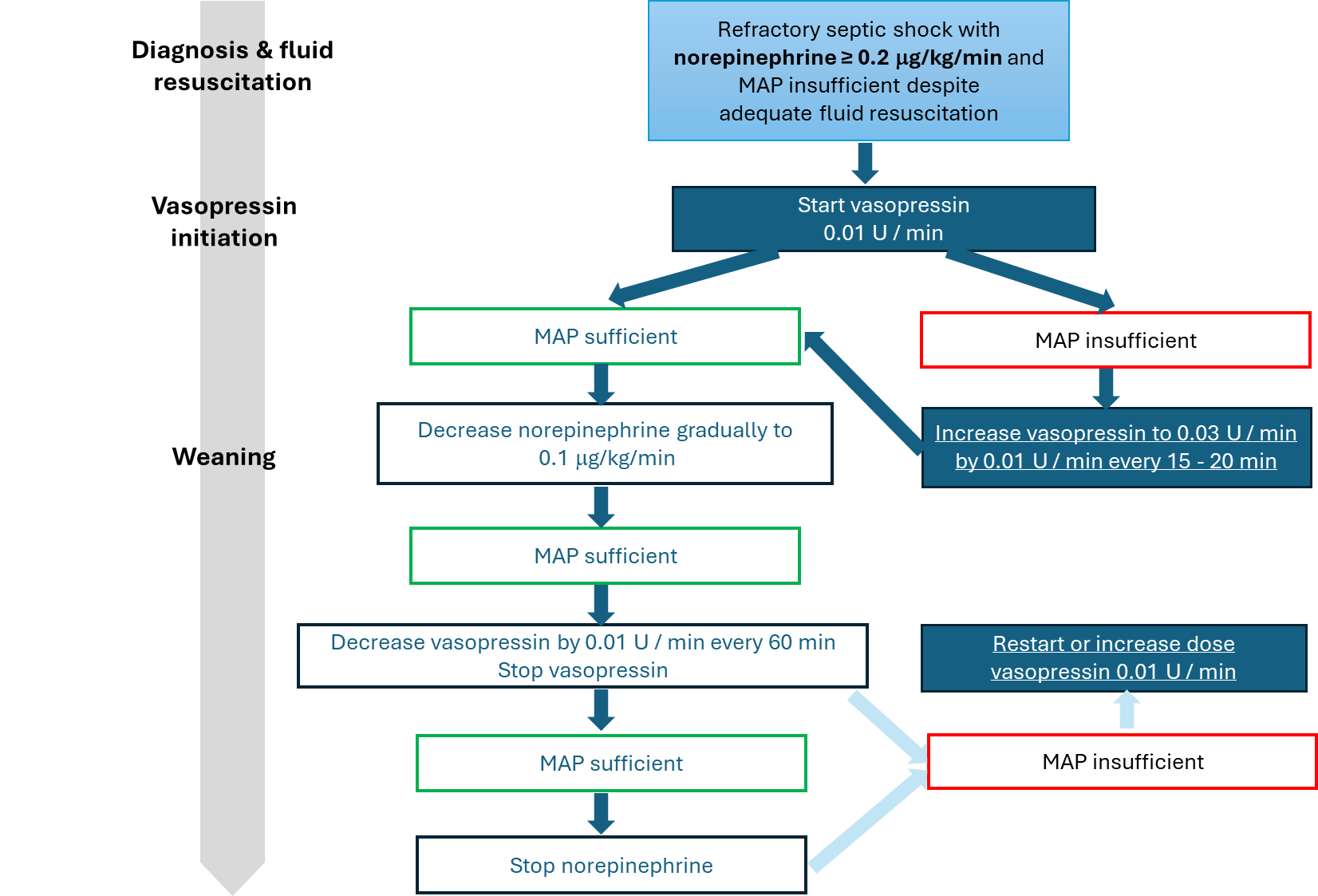
An initiation and dose escalation protocol has been proposed by van Zanten et al.68 It recommends starting vasopressin at 0.01 U/min if MAP remains inadequate (<65 mmHg) despite a norepinephrine dose of 0.20 μg/kg/min, assuming adequate fluid resuscitation and confirmed preserved cardiac output through advanced hemodynamic monitoring (non-invasive and/or invasive).68 If MAP remains insufficient, vasopressin can be increased by 0.01 U/min every 15–20 minutes up to a maximum of 0.03 U/min,68 consistent with the Swiss SmPC of Empressin®.23 However, this titration approach remains empirical and has not yet been validated by randomized controlled trials.
The concept of adjusting vasopressin dosing according to body weight has been investigated in retrospective analyses, yielding conflicting results. Miller et al. (2022) observed that weight-adjusted vasopressin dosing correlated with reduced catecholamine requirements,69 whereas Torbic et al. (2018) found no significant association between body mass index (BMI) and hemodynamic response to fixed-dose vasopressin therapy.70 These discrepancies underline the need for prospective studies to clarify whether weight-based dosing could optimize clinical outcomes.
Weaning
The question of whether norepinephrine or vasopressin should be tapered first during the recovery phase of septic shock remains a matter of ongoing debate.71 Given its longer half-life, tapering vasopressin first may appear physiologically reasonable.72 However, abrupt discontinuation of vasopressin may lead to significant hypotension due to its impact on vascular tone, particularly in the splanchnic circulation.73 Four retrospective cohort studies reported a higher incidence of hypotension when vasopressin was withdrawn before norepinephrine.74–77 This finding was further supported by a retrospective study by Musallam et al., which showed a significantly higher incidence of hypotension (62.2% vs 28.6%; p=0.004) when vasopressin was stopped first. Multivariate analysis confirmed that stopping vasopressin first is an independent predictor of hypotension (OR: 7.2).78
In contrast, a retrospective analysis by Sacha et al. (2018) found no clear benefit of either tapering sequence.79 The DOVSS trial, a small prospective, randomized single-center study, suggested that discontinuing norepinephrine first may be associated with more frequent hypotension.80 A systematic review with meta-analysis81 and two further meta-analyses82,83 found that tapering norepinephrine before vasopressin was associated with fewer hypotensive events, although no differences in mortality or ICU length of stay were observed.81–83 The protocol proposed by van Zanten et al.68 recommends reducing norepinephrine gradually to 0.1 μg/kg/min once MAP is stable, followed by vasopressin tapering in increments of 0.01 U/min every 60 minutes. During this process, careful hemodynamic monitoring is essential to detect and manage rebound hypotension. If MAP falls and cardiac output remains adequate, reinitiating or increasing vasopressin is preferred over escalating norepinephrine.68 However, given the absence of large-scale trials, the optimal weaning strategy remains uncertain; individualized decision-making based on patient response is essential.
Treatment algorithm
The updated treatment algorithm depicted in Figure 1 outlines key updates from the 1st Swiss Vasopressin Consensus, including earlier initiation (at norepinephrine ≥0.2 μg/kg/min), structured dose escalation (0.01 to 0.03 U/min) and a defined weaning sequence prioritizing norepinephrine tapering before vasopressin. This approach aims to enhance hemodynamic stability, minimize rebound hypotension and reduce overall catecholamine exposure.

Vasopressin in other clinical indications
The expert panel evaluated which patient populations may benefit from the vasopressin treatment algorithm. Building upon the discussions from the 1st Swiss Vasopressin Consensus,85 the panel considered both established and emerging clinical settings. While septic shock remains the core indication, potential benefits were also discussed for patients with vasoplegic syndrome following cardiac surgery, acute RV failure and vasoplegia associated with acute liver failure.
Based on the available evidence and expert consensus, the patient populations were categorized into core indications, possible indications and situations where vasopressin is not recommended. A summary of these categorizations is provided in Table 3.
Vasopressin in post-cardiac surgery vasoplegic syndrome with cardiopulmonary bypass (CPB)
Vasoplegia is a well-recognized complication of cardiopulmonary bypass (CPB), affecting 9–44% of patients and associated with mortality rates of up to 25%.86 Its pathophysiology resembles sepsis-induced vasodilatory shock, although the initiating factors and mediators may differ. Patients typically present with profound vasodilation, low systemic vascular resistance, hypotension despite high cardiac output and poor responsiveness to fluids or catecholamines.87–89 During CPB, blood contact with foreign surfaces triggers inflammatory and coagulation cascades, leading to cytokine release, nitric oxide (NO), prostacyclin and other vasoactive mediators that exacerbate vasodilation and hemodynamic instability.90
A 2021 consensus statement from cardiovascular intensive care experts recommends norepinephrine and/or vasopressin to maintain systemic perfusion pressure, with vasopressin as a potential first-line option, particularly in patients with norepinephrine-induced tachyarrhythmias. Standard practice suggests initiating vasopressin when norepinephrine exceeds 0.2 μg/kg/min. In patients with pulmonary hypertension or RV dysfunction, vasopressin may be used as monotherapy or in combination with norepinephrine.91
The VANCS trial compared vasopressin (0.01–0.06 U/min) as a first-line agent to norepinephrine (10–60 µg/min) in 330 patients with vasoplegic syndrome post-cardiothoracic surgery (coronary artery bypass graft surgery, valve replacement, or repair surgery with cardiopulmonary bypass [CPB]).53 Vasopressin significantly reduced the composite outcome of death or severe complications, mainly through lower rates of atrial fibrillation (63.8% vs 82.1%; p=0.0004) and acute renal failure (32.2% vs 49%; p=0.0014). The authors conclude that vasopressin may be an effective first-line vasopressor for post-cardiac surgery vasoplegic syndrome, potentially leading to improved clinical outcomes.53
Several randomized controlled trials have further investigated vasopressin in cardiac surgery settings. A meta-analysis by Dünser et al., including eight RCTs and 625 patients, found that vasopressin reduced perioperative complications, particularly vasodilatory shock and new-onset atrial fibrillation, increased MAP, reduced norepinephrine requirements and did not increase mortality or ischemic events.92
In clinical practice, vasopressin is commonly titrated up to 0.04 U/min postoperatively to restore physiological vasopressin levels.89 However, escalation beyond 0.04 U/min remains empirically based and offers uncertain benefit, while potentially increasing the risk of peripheral or mesenteric ischemia.93 Retrospective studies have associated vasopressin doses above 0.04 U/min with a higher risk of renal dysfunction.94 Nonetheless, doses around or exceeding 0.06 U/min are frequently used in cases of refractory vasoplegia as an alternative to further catecholamine escalation.89
Vasopressin in acute right ventricular failure/cardiogenic shock
Acute right-ventricular (RV) failure is a distinct form of cardiogenic shock, accounting for approximately 5–10% of cases.95,96 It is characterized by impaired RV function leading to reduced left-ventricular preload, diminished cardiac output and systemic hypoperfusion.97,98 Unlike classical vasodilatory shock, acute RV failure is typically not associated with low systemic vascular resistance (SVR) and vasopressors like vasopressin are therefore not routinely indicated solely to increase SVR.98,99 In conditions such as pulmonary hypertension or acute pulmonary embolism, right atrial dilatation may promote the release of atrial natriuretic peptide (ANP), contributing to secondary vasodilation and systemic hypotension.100 In this context, vasopressin may be considered to support perfusion pressure due to its favorable profile on systemic vascular resistance without significantly increasing pulmonary vascular resistance.99,101 However, increasing afterload in the presence of left-sided underfilling may paradoxically impair organ perfusion, particularly if RV contractility is compromised.100 In cases of refractory hypotension, vasopressors such as vasopressin may serve as a bridging therapy until mechanical circulatory support (MCS) can be initiated.98,102
One advantage of vasopressin from the pharmacodynamic point of view lies in its selective systemic vasoconstriction, which raises MAP without significantly increasing pulmonary vascular resistance (PVR) – as demonstrated in a human in vitro model – and which could potentially preserve RV function.103 Early clinical observations by Tayama et al. (2007) in a retrospective case series of nine postoperative patients with RV failure and pulmonary hypertension suggested that vasopressin could increase systemic blood pressure without adversely affecting pulmonary pressure.104 An additional potential mechanism involves V1 receptor-mediated nitric oxide release from pulmonary endothelial cells, possibly promoting pulmonary vasodilation – which could particularly be beneficial in RV failure with pulmonary hypertension.105 However, experimental studies indicate that despite its favorable pulmonary vascular profile, vasopressin may negatively affect RV contractility or cardiac output by substantially increasing systemic afterload.106
While randomized data on the use of pulmonary artery catheters (PAC) in vasopressin-guided therapy are lacking, observational studies in cardiogenic shock suggest potential clinical benefit. In a nationwide analysis of 14,635 patients with STEMI-related cardiogenic shock treated with Impella support, Ismayl et al. (2023) reported significantly lower in-hospital mortality in patients monitored with a PAC (adjusted OR: 0.80 [95% CI: 0.67–0.96]; p=0.01).107 Similarly, a large registry study over 15,000 patients with AMI-related cardiogenic shock found higher survival rates (63% vs 49%; p<0.0001) and identified PAC use as an independent predictor of survival (OR: 1.66; p<0.0001).108 Although these data stem from specific mechanical circulatory support contexts, they reflect expert practice patterns and support the rationale for PAC use in complex shock states.107,108
Vasopressin in acute liver failure
Patients with acute liver failure often exhibit severe hemodynamic instability characterized by profound vasodilation, high cardiac output, reduced systemic vascular resistance and relative hypovolemia due to systemic inflammation and endothelial dysfunction.109 Consequently, vasopressor support, continuous renal replacement therapy and pulmonary ventilation are frequently required to maintain adequate MAP and organ perfusion.110
Relative vasopressin deficiency, a phenomenon observed in end-stage liver disease,111 may also contribute to vasoplegia in acute liver failure, similarly to septic shock, suggesting a potential role for exogenous vasopressin to restore systemic vascular tone. However, no randomized studies have evaluated vasopressin or vasopressin analogs specifically in acute liver failure. While vasopressin analogs such as terlipressin have shown efficacy in hepatorenal syndrome by effectively reducing portal pressure.111,112 These results cannot be directly extrapolated to acute liver failure.
Importantly, vasopressin administration markedly constricts the splanchnic circulation, reducing hepatic and portal venous blood flow and thus raises concerns about systemic vasoconstrictive complications such as exacerbation of hepatic ischemia, which have limited its clinical use.113 Animal studies further emphasize this risk, demonstrating significant reductions in mesenteric blood flow with vasopressin administration.57,114 Given the limited evidence base, vasopressin should be used with caution in patients with acute liver failure and always accompanied by close hemodynamic monitoring to mitigate the risk of ischemic complications.
Implementation considerations
Vasopressin has become an established adjunct therapy for septic and vasoplegic shock in many countries. However, its clinical application remains poorly standardized. Studies and surveys reveal considerable heterogeneity in timing, dosing and implementation protocols across hospitals and intensive care units (ICUs). Differences in vasopressin availability, clinician expertise and hemodynamic monitoring further complicate uniform application.116–118
Effective integration into local ICU protocols must consider institutional resources, available hemodynamic monitoring infrastructure and the clinical expertise of treating clinicians. Institutional adaptations, such as adjusting vasopressin initiation thresholds based on local outcomes, may improve resource utilization and patient care. Looking forward, a dynamic, phase-specific adaptation of monitoring and vasopressor strategies, tailored not only to the evolving clinical status but also to institutional capacities, will be increasingly critical to improve patient outcomes.119
Conclusions
The 2nd Swiss Vasopressin Consensus Report provides evidence-informed, practice-oriented recommendations for the use of vasopressin in septic shock and selected vasodilatory states. Septic shock remains the primary indication, while vasopressin may also be considered for post-cardiac surgery vasoplegia, acute RV failure or cardiogenic shock and acute liver failure based on available evidence.
Key rationales for vasopressin use include its catecholamine-sparing effect, which may mitigate norepinephrine-associated adverse effects and its nephroprotective properties, supported by clinical data showing reduced requirements for renal replacement therapy and slower progression of acute kidney injury in selected patient populations.
The panel recommends initiating vasopressin when norepinephrine reaches ≥0.2 μg/kg/min, accompanied by structured dose escalation and individualized weaning strategies. In contrast to the 2021 Surviving Sepsis Campaign guidelines – which suggest a broader norepinephrine threshold of 0.25–0.5 μg/kg/min and provide limited practical guidance – this expert consensus offers structured, physiology-based recommendations to optimize timing, dosing and de-escalation of vasopressin therapy.
By emphasizing an individualized hemodynamic management strategy – characterized by the principle of “vasopressin earlier in, slower out” – this consensus aims to optimize vasopressor therapy and improve outcomes in patients with septic shock and other vasodilatory states.
Glossary of abbreviations and acronyms
aOR: Adjusted odds ratio
CI: Confidence interval
CPB: Cardiopulmonary bypass
ESC: European Society of Cardiology
HR: Hazard ratio
ICU: Intensive care unit
MAP: Mean arterial pressure
RCT: Randomized controlled trial
RR: Risk ratio
RRT: Renal replacement therapy
RV: Right ventricle/right ventricular
SmPC: Summary of Product Characteristics
SSC: Surviving Sepsis Campaign
U: International units
V1a, V1b, V2: Vasopressin receptor subtypes
Conflicts of interest
The author(s) has (have) declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
Preparation of this manuscript and the face-to-face expert panel meeting were funded by OrPha Swiss GmbH. The sponsor had no influence on the final version of the manuscript. The views expressed in this article reflect solely the consensus of the authors based on the available literature, relevant guidelines and the Swiss SmPC for Empressin®.
Author contributions
All authors contributed to and approved the final manuscript.