
Introduction
The pursuit of optimal vitamin D levels poses a significant challenge in healthcare, characterized by numerous uncertainties and complexities, as well as diverse guidelines and recommendations tailored to different populations.1 Clinicians and patients must navigate a convoluted landscape of vitamin D management influenced by changing testing protocols and coverage policies.2,3 This scenario requires thoughtful consideration of various factors, including who should be tested for vitamin D deficiency, the costs associated with testing, when testing is appropriate, and the circumstances that necessitate supplementation.4
In Switzerland, as in many parts of the world, achieving ideal vitamin D levels is a multifaceted and often unclear endeavor.5 The World Health Organization (WHO) defines vitamin D deficiency as serum levels below 20 ng/mL (50 nmol/L), with severe deficiency classified as levels below 10 ng/mL (25 nmol/L).6 Similarly, the Swiss Federal Office of Public Health (BAG) adopts this classification, identifying same deficiency and severe deficiency. Despite these established criteria, the global incidence of vitamin D deficiency remains high, affecting approximately one billion people, with half of the population failing to meet the recommended levels.7
Recent studies suggest that vitamin D deficiency is prevalent across all age groups, with significant disparities based on geographic location, lifestyle, and skin pigmentation.8
Furthermore, vitamin D status is influenced by seasonal variation, with deficiency rates peaking during winter months due to reduced sun exposure.9
In Switzerland specifically, the situation is even more pronounced, as 59% of primary care patients exhibit insufficient vitamin D levels. Among them, 12% are classified as deficient, with serum levels below 20 ng/mL (50 nmol/L). However, the classification criteria for the remaining 47% within the insufficient range are not explicitly defined in the referenced study and may include patients with suboptimal but not deficient levels.10 Furthermore, since July 1, 2022, basic health insurance in Switzerland no longer covers vitamin D testing for individuals without specific risk factors. Currently, reimbursed testing is limited to patients with conditions such as osteoporosis, chronic kidney disease, malabsorption syndromes, and disorders affecting calcium metabolism.11 As we grapple with the complexities of data interpretation and application, the challenge of aligning diverse, sometimes contradictory, recommendations from professional organizations becomes increasingly apparent. For instance, the Swiss Endocrine Society12 recommends a higher threshold for sufficiency (>30 ng/mL or 75 nmol/L) based on its clinical practice guidelines, whereas the Institute of Medicine in Switzerland considers 20 ng/mL (50 nmol/L) sufficient, citing evidence related to bone health.12 This discrepancy underscores the ongoing debate about optimal vitamin D targets and their clinical implications. Additionally, the impact of vitamin D on non-skeletal health outcomes, such as immune function and chronic disease prevention, remains an area of active research.13
Effectively translating guidelines into actionable strategies for optimizing vitamin D levels requires a nuanced approach tailored to individual patient needs. This article aims to address these challenges by a real-world analysis of the effects of vitamin D supplementation on vitamin D levels. Our objective is to empower clinicians with the knowledge and resources necessary to navigate the intricacies of vitamin D optimization, ultimately enhancing informed decision-making and improving patient outcomes.
Method of data collection
Patients from the endocrinology/diabetology outpatient clinic at the DiaMon Institute (Baden-Dättwil, Switzerland), which specializes in diabetology, endocrinology, and obesity, were retrospectively analyzed. The study included patients on continuous oral vitamin D supplementation whose 25-hydroxyvitamin D (25-OHD) levels were measured between August and December 2021 (referred to as the “final level”). These patients had initially been diagnosed with vitamin D deficiency (25-OHD <20 ng/mL) in the preceding 3–12 months, leading to the initiation of supplementation. Patients who had received vitamin D in any form within the six months prior to the baseline measurement were excluded from the study.
To ensure transparency and consistency, the following definitions and classifications for vitamin D levels shown in Table 1 were used in this study.
Oral vitamin D supplementation was administered with depot preparations (such as cholecalciferol 100,000 IU or 300,000 IU) or maintenance doses (including cholecalciferol tablets 1000 IU, cholecalciferol oil 500 IU/drop, cholecalciferol drops 4000 IU/ml, and cholecalciferol capsules 800 IU). Total 25-OHD levels were measured using a Cobas e601 analyzer (Roche) employing an electrochemiluminescence binding assay. This method was standardized against internal standards traceable to the isotope dilution-liquid chromatography-tandem mass spectrometry (ID LC-MS/MS) 25-OHD reference method. Both, the intra- and interassay variation of the assay, was below 7%.
The reference values are based on the recommendations of the Swiss Nutrition Commission, as outlined in the Expert Report.16
The reference values for 25-OHD- on Cobas e601 were as follows: mean, 26.6 ng/ml; median, 25.7 ng/ml (winter, 22.8 ng/ml; summer, 27.7 ng/ml), 2.5th percentile, 10.2 ng/ml; 97.5th percentile, 49.4 ng/ml.
In the first step, we analyzed adequacy in patients who only received maintenance doses (22 patients) and established criteria to assess the response of the vitamin D levels, regardless of individual risk factors.
Adequacy was determined by doses of supplement and amount of delta from the vitamin D values:
a) “Inadequate” and “weak” response were defined as follows:
-
For patients receiving >800 IU/day of vitamin D supplementation: if there was no increase in serum levels of >10 ng/ml.
-
For patients with no increase in serum levels: if the increase was within the 7% measurement precision, regardless of the supplementation dose.
b) “Inadequate” and “strong” response were defined as follows:
- For patients receiving ≤800 IU/day of vitamin D supplementation: if there was an increase in serum levels of >10 ng/ml.
c) “Adequate” response was defined as follows:
- For patients who did not fall into categories (a) or (b).
In the second step, we evaluated unexpectedly weak and strong responses based on risk factors to determine their explainability by analyzing how these factors influenced adequacy:
a) “Inexplicable” response was defined as follows:
-
For weak responses: if <2 risk factors were present (without the strongest risk factor malabsorption) or if there was no increase in serum levels regardless of the number of risk factors.
-
For strong responses: if ≥2 risk factors were present.
b) “Explicable response” included all remaining patients receiving maintenance doses only and who did not fall into the “inexplicable” response category.
Basic data
Of the 261 screened patients, 120 underwent a 25-hydroxyvitamin D (25-OHD) measurement (serum level measurement) between August and December 2021. Among these, 45 patients had a prior measurement within the preceding 3–12 months, and 37 of them were diagnosed with vitamin D deficiency (<20 ng/mL) at baseline (Figure 1).

Nine patients were excluded from the study:
-
2 patients because, despite the deficiency, no vitamin D supplementation was administered.
-
3 patients because the supplementation was interrupted before the final serum level measurement.
-
4 patients because a vitamin D product had been administered immediately before the initial measurement.
Among the 28 patients included according to the vitamin D guidelines of the BAG were:
-
3 patients had a severe vitamin D deficiency (just below 10 ng/ml).
-
16 patients were in the lower range of vitamin D deficiency (10–15 ng/ml).
-
9 patients were in the upper range of vitamin D deficiency (15–20 ng/ml).
Patients were managed by internists and endocrinologists at the DiaMon Institute, ensuring expertise in vitamin D metabolism and related conditions.
Nine patients were externally referred from general practitioners to the DiaMon Institute, while 19 were referred internally from the general practice affiliated with the DiaMon Institute. None of the patients were referred specifically for vitamin D deficiency; rather, they were seen for various endocrinological or metabolic concerns.
The identified risk factors for vitamin D deficiency among these patients are summarized in Table 2.
The average age was 56.3 years (range, 20–84; standard deviation [SD], 18.2). The average weight was 84.9 kg (range, 47.9–131; SD, 9.3). The average body mass index (BMI) was 30.2 kg/m² (range, 17.2–48; SD, 6.5).
In 11 patients, the initial and final vitamin D levels were measured in different seasons (summer/winter). All values were standardized to winter values (October-April) according to the assay’s reference values.
Results
Substitution doses
Four patients initially received oral depot vitamin D (depot) without daily maintenance doses, with an average dose of 150,000 IU (range: 100,000–230,000; SD: 57,155). Two patients received a second depot dose following an intermediate measurement. Maintenance doses were administered in 24 patients, with two also receiving an initial depot dose. The average daily maintenance dose was 871 IU (range: 500–1600; SD: 308). The maintenance dose was prescribed from the first measurement of the initial vitamin D level to the final level. In two patients, the maintenance dose was increased after an intermediate measurement.
The three patients with severe vitamin D deficiency (<10 ng/mL), received a maintenance dose of 800 IU, and one patient received an initial depot dose of 100,000 IU. For the 16 patients with vitamin D levels in the lower range of deficiency (10–15 ng/mL), the average maintenance dose was 873 IU (range, 500–1600; SD, 296), and two patients received depot doses of 100,000 IU and 200,000 IU, respectively. For the nine patients with vitamin D levels in the upper range of deficiency (15–20 ng/mL), the average maintenance dose was 879 IU (range, 500–1428; SD, 347). Additionally, three patients received depot doses of 100,000 IU, 230,000 IU, and 150,000 IU, respectively.
Risk factors
On average, each patient presented with 1.29 risk factors (range, 0–4; SD, 1.08). Seven patients exhibited no identifiable risk factors. In total, nine of the risk factors outlined in the introduction were observed (Table 2). The following risk factors were not identified in this cohort: medications, liver insufficiency, pregnancy/lactation, chronic inflammation (excluding chronic pancreatitis, which was categorized as malabsorption), and active bone fractures.
Poorly controlled diabetes (17 cases) and thyroid disorders (7 cases) were excluded as risk factors, as all patients achieved significant improvement in HbA1c and euthyroidism before the final vitamin D level measurement.
We included also primary hyperparathyroidism because low 25-OHD levels in these patients are frequent, because the production and metabolism of 25-OHD is downregulated as a protective mechanism, since blood does not require additional calcium.
Vitamin D levels (initial, intermediate and final)
The timing of vitamin D level measurements varied significantly, influenced by follow-up appointments for diabetes, thyroid disorders, or other endocrinological conditions. Poor adherence to supplementation, particularly for maintenance doses, may also explain some unexpected trajectories. Additionally, the COVID-19 pandemic likely altered patients’ sun exposure patterns, further complicating the assessment.
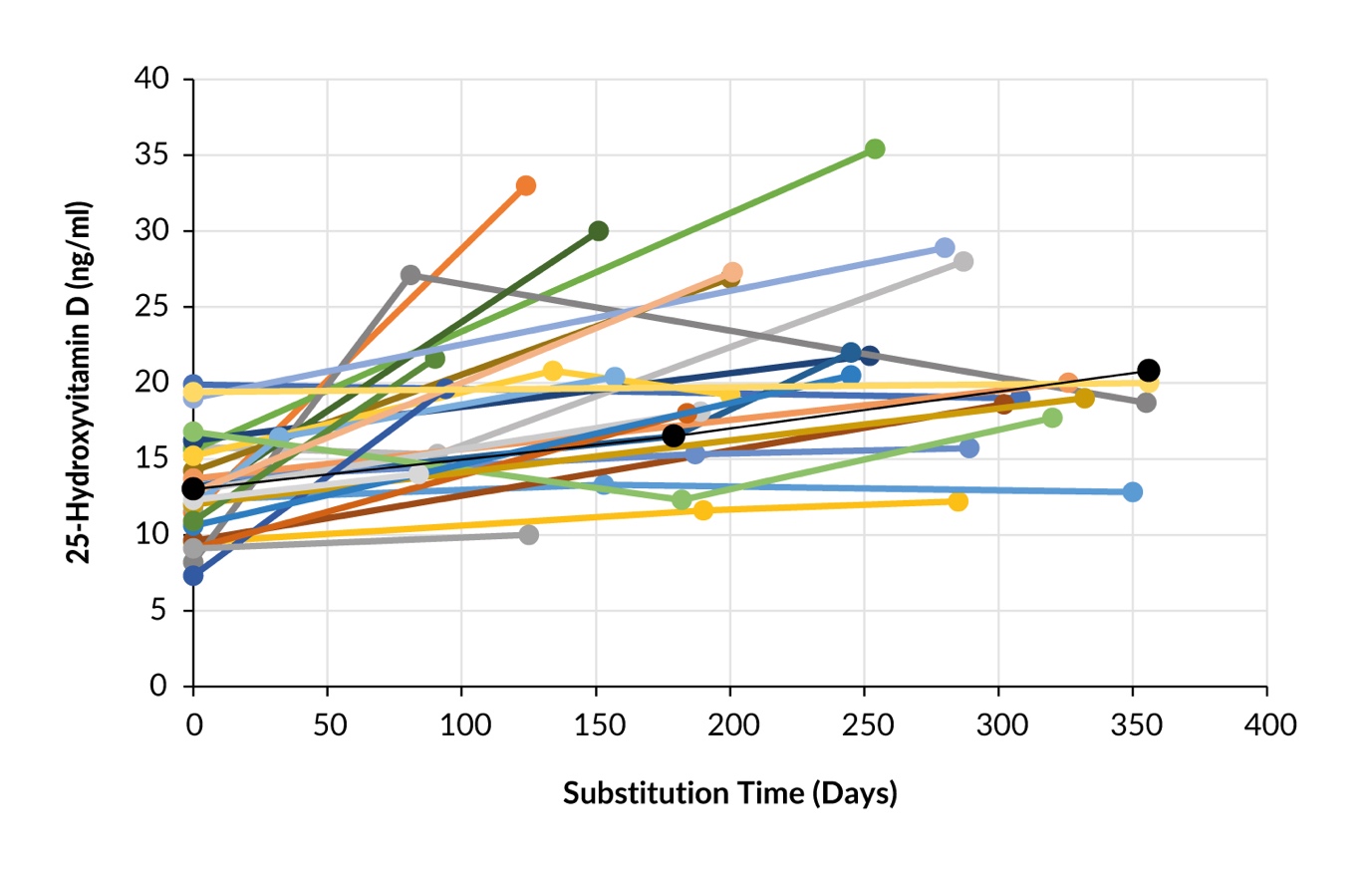
Figure 1 shows the changes in the vitamin D levels over time for each patient. The average initial level was 13.0 ng/ml (range, 7.3–19.9; SD, 3.3) and the average final level was 20.8 ng/ml (range, 10.0–35.4; SD, 5.8). The average intermediate level measured in nine patients was 17.5 ng/ml (range, 11.6–27.1; SD, 4.8). At the final measurement, 14 patients still had deficiency levels of <20 ng/ml, while 14 patients reached the target level of >20 ng/ml. Among these, three patients achieved levels >30 ng/ml.
Intervals between measurements
The average duration between the initial and final vitamin D measurements was 234 days (range, 84–356; SD, 85). For nine patients, an intermediate measurement was taken after 2–4 months.
Delta between initial, intermediate and final levels
The average delta between the initial and final levels was +7.7 ng/ml range, -2.2–19.8; SD, 5.6). Five patients had no change in their initial levels within the 7% measurement precision of the assay. In total, 23 patients experienced an increase between the initial and final levels (Figure 2).

Key findings from Figure 2:
-
28 patients with vitamin D deficiency (1.8 risk factors on average).
-
Maintenance dose 871 mg/day on average.
-
Six patients received a depot of 150,000 IU on average.
-
Black line indicates the average increase by 7.7 ng/ml.
-
Overall, very individual and varied responses were observed, with some surprisingly high/low responders.
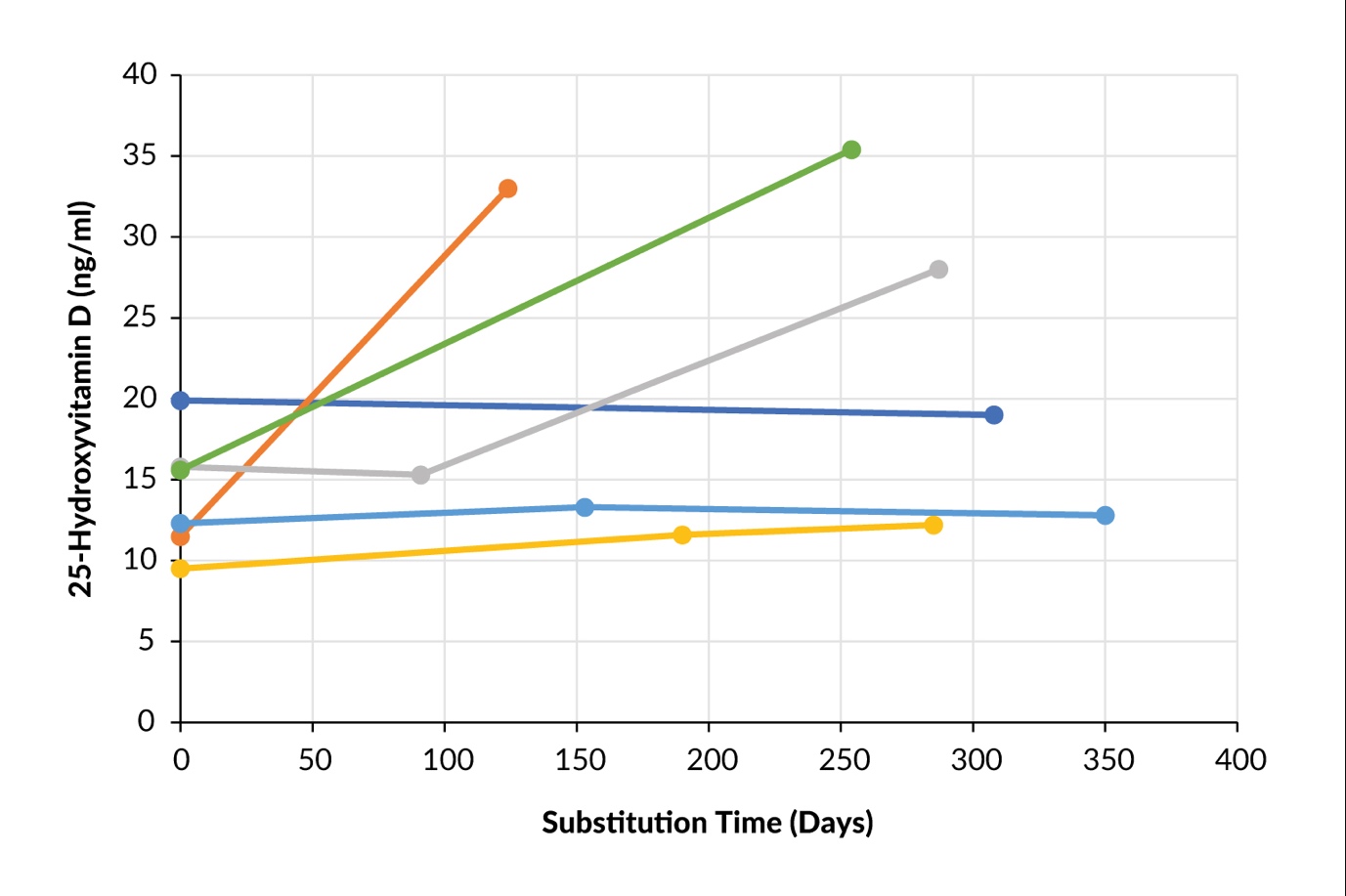
For six patients receiving daily maintenance doses, an intermediate measurement was taken, and all showed an increase. In one of the four patients who received only depot doses, the intermediate level was lower than the initial level (Figure 3).
Supplementary analysis revealed that among patients with weak responses, it was defined as an increase of less than 10 pg/ml in 25-OHD D (n=19) – the number of risk factors per patient ranged from 0 to 4, with a mean of 1.1 (SD, 1.3). In contrast, patients with strong responses – an increase of more than 10 pg/ml (n=9) – had risk factors ranging from 0 to 3, with a mean of 0.7 (SD, 1.0). Notably, malabsorption was identified as a strong risk factor in 3 patients from the weak response group compared to only 1 patient in the strong response group.

Key findings from Figure 3:
-
Two patients (orange/green) with sufficient increase in vitamin D levels with correct depot and maintenance dose.
-
One patient (gray) with 2x depot substitution without maintenance dose; sufficient increase only after intermediate level following a higher second depot.
-
One patient (dark blue) with no increase despite 100,000 units depot (at start and intermediate measurement) plus maintenance dose 1000 IU/day; since only one risk factor (BMI per magna with 42 kg/m2) was present, representing an unexplained course.
-
One patient (light blue) with no increase, since only depot without maintenance dose; intermediate measurement after depot missed, assessment of adequacy therefore not possible.
-
One patient (yellow) with no increase despite depot, no maintenance dose; since the intermediate measurement was late, it is not assessable whether there was an adequate increase. No second depot was administered after the intermediate measurement, and the level did not change.
Patients on depot doses
Depot doses were administered to a total of six patients (21%): once for a vitamin D level <10 ng/ml, three times for levels 10–15 ng/ml and twice for levels 15–20 ng/ml. Among those receiving vitamin D depot doses, only two of the six patients had an intermediate measurement taken at the optimal interval of three months for assessment.
According to Figure 2:
-
Three patients had an increase to >20 ng/ml.
-
One patient had no increase.
-
Two patients with only depot doses could not be assessed because the measurement was performed too late.
Patients on maintenance dose only
Of the 22 patients who were on maintenance doses only, six patients experienced an increase in vitamin D levels of >10 ng/mL, while 16 patients had an increase of <10 ng/mL. Nine patients received a maintenance dose of >800 IU/day, while 13 patients received a dose of ≤800 IU/day.
Using the definition of adequate or inadequate response to vitamin D supplementation mentioned in the data collection method, we identified nine patients with a weak response and four patients with a strong response. According to the definition of explainability, we found that two of the four strong responses and six of the nine weak responses were inexplicable (see Table 3).
Reactions in patients on maintenance dose only
Weak responses were in 9 patients, number of rheumatoid factor (RF) 0–4, mean 1.1 and SD ±1.3.
Strong responses were in 4 patients, number of RF 0–3, mean 0.7 and SD ±1.
The strongest RF (malabsorption) was observed in 3 patients in the “weak response” group and in 1 patient in the “strong response” group.
In 10 of the 13 patients receiving 800 U/day despite the low vitamin D level, the response was strong, 2 of them had even a strong RF (malabsorption), the number of RF was 0–3, mean 0.8 and SD ± 0.9.
In summary, out of the 22 patients with maintenance doses, 8 (36.3%) had an inexplicable reaction (27,2% inadequate weak, 9.1% inadequate strong) and 14 (63.7%) had a explicable reaction (13.7% inadequate weak, 9.1% inadequate strong, 40.9%), see Table 3.
Recommendations
Based on these findings, we recommend initially administering a depot dose to address potential adherence issues, followed by a maintenance dose tailored to the identified risk factors. After three months (approximately five half-lives of 25-OHD), the effect of the depot dose should be assessed. If levels normalize, a second measurement after three months can help evaluate the appropriate daily maintenance dose.
Discussion
In this study, 261 patients were selected from an endocrinology clinic based on predefined inclusion criteria rather than true randomization, ensuring representation of individuals undergoing vitamin D assessment in routine clinical practice. Among them, 120 patients (46%) underwent vitamin D measurement, reflecting the high rate of testing in patients with diabetology, endocrinology, and obesity-related conditions, rather than directly indicating a high prevalence of deficiency.
Of the 28 patients diagnosed with vitamin D deficiency that were studied, 21 (75%) had at least one established risk factor for vitamin D deficiency. After supplementation, 23 patients (82.3%) showed an increase in 25-OHD levels, though with considerable variability (Figure 2). However, in five patients (17.8%), vitamin D levels remained unchanged, suggesting potential issues with adherence or strong malabsorption, or other unknown reasons like metabolic resistance.
Overall, 11 patients (39%) reached levels between 20–30 ng/ml, still considered inadequate according to the BAG7 while only three (10.7%) achieved levels >30 ng/ml. Two of these were in the depot group and one in the maintenance-only group. Patients received an average supplementation dose of 871 IU/day, only slightly above the BAG-recommended maintenance dose for individuals over 60. Given the cohort’s risk factors (mean 1.23 per patient), this dose was likely insufficient and should have been adjusted accordingly.17 Risk-based dose adjustments improve outcomes, but remain underutilized in clinical practice.18
Notably, patients with mild vitamin D deficiency (10–20 ng/ml) received a higher mean dose than those with severe deficiency, suggesting inconsistent application of BAG guidelines.19 Such inconsistencies have been observed in various healthcare settings due to a lack of consensus on optimal strategies.20 The six patients receiving depot preparations are detailed separately in Figure 3.
Among the 22 patients on maintenance doses, responses varied:
-
18% (4/22) had unexpectedly strong responses.
-
41% (9/22) had unexpectedly weak responses.
-
41% (9/22) showed adequate increases.
-
59% (13/22) showed inadequate changes in their vitamin D levels.
A detailed qualitative assessment of risk factors (Table 2) proved challenging due to ambiguous effects on vitamin D metabolism, such as renal insufficiency, obesity, and skin color. Only malabsorption (two patients) was consistently identified as a strong risk factor. Gastrointestinal disorders have been reported to significantly impair vitamin D absorption, necessitating higher supplementation doses.21
In eight patients (36%), unexpected changes in vitamin D levels remained unexplained. These were mostly weak responders (6/9) but also included two strong responders. Possible causes include inadequate measurement intervals, influenced by regular follow-ups for diabetes or thyroid disorders, where vitamin D was not the primary focus.22 Timing of measurements matters, particularly in the maintenance dose group, as deficiencies may resolve over time, requiring dose adjustments.23 Adherence to supplementation is another challenge—monitored for depot doses but difficult to verify for maintenance therapy.24 Poor adherence is generally a key barrier in at-risk populations.25
Poor adherence is a well-documented challenge across various patient populations, particularly those at higher risk for vitamin D deficiency. Factors such as complex supplementation regimens, lack of awareness, and inconsistent follow-up contribute to suboptimal treatment outcomes.23 Ensuring adherence to vitamin D therapy in private practice is challenging. Consequently, administering vitamin D intramuscularly or orally under direct supervision is advisable.
Additional factors complicating vitamin D assessments include individual variability in metabolism, malabsorption, dietary intake, sun exposure, and skin pigmentation.26 In our cohort, eight patients (28.5%) had darker skin, making it difficult to estimate their reduced cutaneous vitamin D synthesis.5 This aligns with research showing higher supplementation needs in darker-skinned individuals.27 The COVID-19 pandemic may have further altered sun exposure patterns.
Changes in underlying health conditions can also affect vitamin D status. For instance, improvement in renal insufficiency or discontinuation of interfering medications can alter levels. While obesity remains a stable risk factor, diabetes and thyroid disease were excluded due to their potential for rapid fluctuations. Seasonal variation further complicates assessment — 39% of patients showed seasonal differences, with vitamin D levels averaging 18% lower in winter.28 These findings underscore the need for seasonally adjusted supplementation.
Even with optimal monitoring, adherence checks, and guideline-based dosing, some trajectories remain unexplained due to individual differences in vitamin D metabolism.
Given these complexities and based on our findings, we recommend:
-
Administer an initial depot dose to address potential adherence issues, followed by a maintenance dose tailored to identified risk factors.
-
Assess the effect of the depot dose after three months (approximately five half-lives of 25-OHD).
-
If levels normalize, perform a second measurement after three more months to evaluate the appropriate daily maintenance dose.
Our retrospective study has some limitations. The fact that 25-OHD measurements and vitamin D supplementation was sometimes given out of known indications reflects the real- world situation in clinics and maybe the pression of patients for such activities, which are not always indicated.
Because of the retrospective analyses of this real-world clinical study, the implemented indications and strategies for substitution and some variables were not controlled. Vitamin D deficiency was always only a side problem in the analyzed contact between patients and doctors. Therefore, the few analyzed parameters are maybe not sufficient to explain reasons for a missing success in the determination of vitamin D doses. Measurement of other parameters in vitamin D metabolism (calciuria, calcemia, phosphatemia, intact PTH or others) may have helped to optimize substitution.
Since 2022, Switzerland has imposed limitations on the reimbursement for vitamin D testing, according to the analysis list for certain risk situations and intervals between follow-up examinations.11 Given the number of risk factors, the difficulty of assessing them and their dynamic nature, the success of supplementation depends on a clinical approach and continuous reassessment of the correct therapeutic dose. Vitamin D measurements, together with a thorough patient history, will help in this process. In cases of vitamin deficiency, it may sometimes be sufficient to inquire about the patient’s habits and potentially improve them. In cases of an inadequate response to supplementation, therapy adherence should also be addressed.
Conclusion
This study reveals that current vitamin D supplementation practices often fail to achieve optimal serum vitamin D levels, especially among individuals with baseline deficiency. Only 40% of participants with initial vitamin D levels between 10–20 pg/mL reached the target range of 20–30 pg/mL, a range that still falls below the recommended thresholds as per BAG. Furthermore, only 10% of the individuals achieved an ideal level of 30–50 pg/mL, suggesting that typical dosing regimens are insufficient for many individuals.
The factors contributing to these suboptimal outcomes include ongoing debates within the medical community regarding the clinical importance of mild vitamin D deficiency and inconsistent standards for defining optimal vitamin D levels. Additionally, the study highlights significant variability in vitamin D levels among patients receiving maintenance doses; 36% of the patients analyzed showed fluctuations despite receiving presumed appropriate doses and accounting for known risk factors. This variability may stem from practical challenges encountered in real-world settings, including infrequent vitamin D measurement intervals, insufficient initial consideration of individual risk factors for deficiency, evolving risk factors after therapy initiation and limited adherence to supplementation protocols.
To address these issues, it is recommended that clinicians strictly follow the BAG guidelines, combining appropriate maintenance doses with an initial depot (bolus) dose for patients. A follow-up assessment of vitamin D levels should be performed after three months to evaluate the efficacy of the bolus dose, followed by a second evaluation three months later to assess the effectiveness of the maintenance dose, assuming that initial levels have increased sufficiently. Proper accounting for the impact of individual risk factors remains essential and complex, underscoring the need for a personalized approach.
These findings underscore the necessity for a more rigorous and tailored approach to vitamin D supplementation. Improved clinical outcomes are achievable through precise dosing, regular serum level assessments, and personalized interventions that take individual patient risk profiles into account. This comprehensive strategy would facilitate better management of vitamin D deficiency, promote adherence and ultimately enhance patient health outcomes.
Ethical considerations: Consent and privacy
This study was conducted in accordance with the principles of the Declaration of Helsinki. Due to the nature of the study, specific written informed consent for participation was not obtained. However, all patient information was anonymized to maintain privacy, and the study adhered to the ethical standards for the use of patient data in research and publication.
Availability of data and materials
All patient data that support this study/case report are included in the anonymized form in the published article.
Conflict of interest
The authors have declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.