_of_our_patient_showing_pulmonary_nodules_suggestive_of_.tiff)

Introduction
Cryptococcosis, caused by the pathogenic yeast Cryptococcus spp. (mainly Cryptococcus neoformans), represents the third most frequent invasive fungal infection in solid organ transplant (SOT) recipients1 and is associated with high mortality rates. Its diagnosis and treatment are challenging, and studies are lacking in this population. The current therapeutic approach, based on an initial induction regimen (e.g., amphotericin B and flucytosine) followed by a maintenance regimen (e.g. fluconazole) is associated with toxicity and potential drug-drug interactions.2 We present here a case of disseminated cryptococcosis in a lung transplant recipient with renal insufficiency who was successfully treated with an alternative regimen using fewer doses of amphotericin B in order to limit nephrotoxicity.
Case presentation
In March 2022 a 67-year-old woman presented to the pulmonology clinic with a 10-day history of malaise, fatigue and weight loss, associated with a runny nose, a low-grade fever and a non-productive cough. She underwent double lung transplantation in 2011 for lymphangioleïomyomatosis and suffered from chronic lung graft dysfunction of grade 3 and a phenotype of bronchiolitis obliterans syndrome (BOS). She was on an immunosuppressive regimen of tacrolimus, everolimus and prednisone (7.5 mg per day). Additional medical history included hypertension, chronic kidney disease with an estimated glomerular filtration rate (eGFR) of 35 ml/min/1.73 m2, atrial fibrillation and several episodes of viral and bacterial respiratory tract infections since transplantation.
During outpatient consultation, she mentioned a worsening of her symptoms, with diffuse myalgia, headache and intermittent low-grade fever every 2–3 days. She denied any travel or contact with sick persons. On physical examination, she had a blood pressure of 129/78 mmHg, a heart rate of 80/minute and oxygen saturation of 97% on ambient air with a normal respiratory rate and a temperature of 37.2 °C. The physical examination was unremarkable, including a normal neurological examination and no cutaneous or mucosal lesions.
Laboratory tests revealed a total leukocyte count of 8200 cells/µL, with an absolute neutrophil count of 4920 cells/µL, total lymphocytes at 1390 cells/µL, no eosinophilia, slight anemia with a hemoglobin of 117 g/L and a normal thrombocyte count. Natremia was 128 mmol/L with normal kaliemia. There was a worsening of renal function with a serum creatinine of 229 µmol/L (eGFR of 16 ml/min/1.73 m2) compared to baseline serum creatinine values between 200 and 215 µmol/L. C-reactive protein was 23 mg/L. Liver function tests were within the normal range. Chest X-ray showed only a small left-sided pleural effusion, unchanged from previous images. Naso-pharyngeal swabs polymerase chain reaction (PCR) testing was negative for SARS-COV-2, influenza virus and respiratory syncytial virus (RSV). Two pairs of blood cultures were taken. Due to her good overall state, the patient was sent home while awaiting the remaining microbiological results.
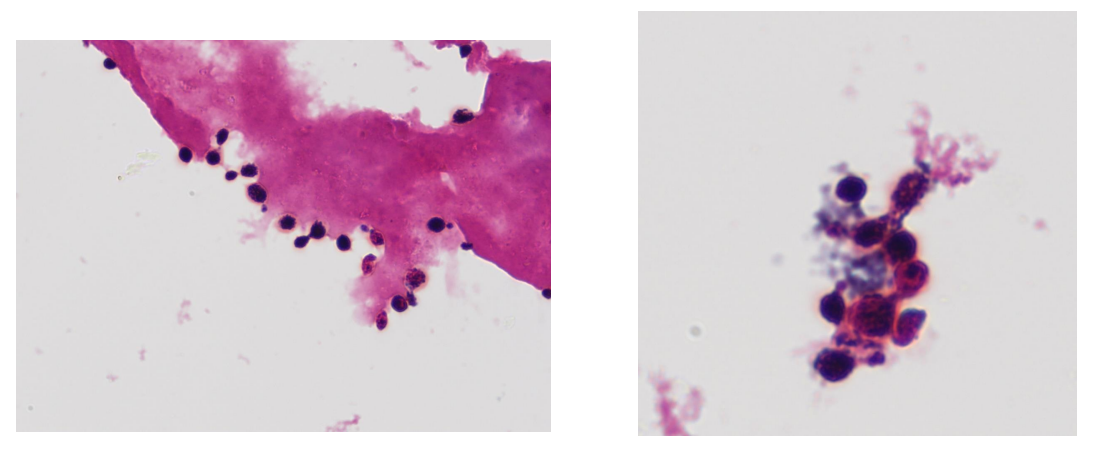
Five days after her consultation, the blood cultures grew round, non-filamenting yeast-like organisms, as shown in Figure 1, that were suggestive of Cryptococcus spp.

The patient was hospitalized as soon as blood culture results became available, and IV fluconazole 400 mg was administered pending formal identification of the pathogen. On hospital admission, she mentioned an increased headache intensity. Serum cryptococcal antigen (CRAG) came back highly positive at 1/5120. The yeast identified in the blood cultures was confirmed to be C. neoformans by Matrix Assisted Laser Desorption Ionization – time of flight (MALDI-TOF) analysis. A lumbar puncture (LP) showed a normal opening pressure and a cerebrospinal fluid (CSF) with elevated leukocytes of 69 cells/µL with neutrophils of 44% and lymphocytes of 42%, increased proteins at 650 mg/L, glucose at 2.4 mmol/L and elevated lactates at 3.32 mmol/L. The CRAG was also increased in the CSF, and the CSF culture grew C. neoformans.
A non-contrast full-body computed tomography (CT)-scan showed peribronchovascular condensations in the lingula with nodules and micronodules (Figure 2). There were no other abnormalities on abdominal and head CT, with no signs of increased intracranial pressure.
_of_our_patient_showing_pulmonary_nodules_suggestive_of_.tiff)
The diagnosis of disseminated cryptococcosis with fungemia, meningitis and pneumonia was made.
Because of the important renal dysfunction and the potential nephrotoxicity of liposomal amphotericin B (L-AmB), there was a concern to start standard treatment of cryptococcosis according to the Infectious Diseases Society of America (IDSA) 2010 guidelines, which recommend an induction therapy combining IV L-AmB with flucytosine for two weeks.2 Therefore, we adhered to a therapeutic regimen derived from a very recent randomized controlled trial showing the non-inferiority of induction treatment with single high dose L-AmB (10 mg/kg) combined with 14 days of IV flucytosine at 100 mg/kg/day in four divided doses and fluconazole 1200 mg/day compared to the World Health Organization (WHO) recommended therapy of amphotericin B deoxycholate and flucytosine for seven days, followed by fluconazole 1200 mg for seven days3 for the treatment of cryptococcal meningitis in adult patients with human immunodeficiency virus (HIV).
The patient received the first dose of IV L-AmB at 10 mg/kg on day 1, with IV flucytosine adapted to her renal function at a dose of 25 mg/kg every 24 hours for 14 days and oral fluconazole, adapted to 600 mg per day. Due to the disseminated disease, we decided to administer another dose of 10 mg/kg of L-AmB on day 7. Dosages of tacrolimus and everolimus were adapted according to therapeutic drug monitoring, taking into account drug-drug interactions.
Follow-up blood cultures were sterile on day 3 of treatment. An LP was done on day 15, which showed normal opening pressure, a decrease in leukocyte counts and CSF proteins, as well as no growth of C. neoformans. CRAG was still positive in the serum, with lower titers (1/5120 on day 1, 1/2560 on day 15) and in the CSF (quantification not done). The patient improved clinically: the fever stopped on day 3, and the headache diminished progressively. Renal function remained stable during treatment. After the results of the second LP performed on day 26, the patient was switched to consolidation therapy with oral fluconazole 400 mg per day (dose adapted for renal function). The timeline of the patient treatment and evolution is presented in Figure 3. The consolidation therapy was continued for eight weeks according to IDSA guidelines recommendations and was then switched to maintenance therapy with fluconazole 200 mg per day.2

The patient recovered from cryptococcosis but had a prolonged hospitalization due to the acquisition of nosocomial SARS-CoV-2 complicated with bacterial superinfection. She was discharged three months after admission. In the following months, she had further deterioration of her pulmonary and renal function, which required the start of dialysis. Due to worsening quality of life, she opted for a palliative approach and died one year after the diagnosis of cryptococcosis, with no signs of disease recurrence.
Discussion
Cryptococcosis is an invasive fungal infection caused primarily by two species of encapsulated yeasts, Cryptococcus neoformans and Cryptococcus gattii.4,5 It can occur in immunocompetent hosts, but most cases occur in immunocompromised hosts, mainly persons living with HIV suffering from acquired immunodeficiency syndrome (AIDS), but also in SOT recipients. Cryptococcosis is estimated to be the third cause of invasive fungal infection after transplantation, with an estimated incidence ranging from 0.2% to 5%4,6 and high mortality rates (5–20%).4,7
C. neoformans is found in the environment (soil, trees) and in bird feces. Patients get infected mainly through inhalation of the microorganism from environmental sources, with infection in SOT recipients estimated to be mainly caused by reactivation of a quiescent infection.8 However, primary infection after transplant and cases of donor-derived infections have been described.4,9 In general, cryptococcosis is considered a late-occurring infection in SOT, with a median time to onset of disease between 16 and 21 months.4,10,11 In that aspect, our case was unusual, with an infection occurring 11 years after transplantation.
Most infections with C. neoformans involve the central nervous system (CNS) or the lung. Clinical presentation is often insidious and non-specific, as was the case in our patient. In patients with meningitis, prolonged headaches, fever, malaise and altered mental status are described, but usual signs of meningeal irritation such as nuchal rigidity are often absent. Pulmonary infection is also common, with symptoms ranging from asymptomatic pulmonary colonization to severe pneumonia with respiratory failure. Radiologic findings of pneumonia are frequently solitary or multiple nodules, and the differential diagnosis should include other invasive fungal diseases. Other sites of infection include skin, bone, joints and more rarely liver, kidney and prostate.4 In SOT patients, disseminated or extrapulmonary disease at the time of diagnosis is frequent (50–75% of cases).4,12 Therefore, fungemia and CNS involvement should always be actively looked for in SOT patients with cryptococcosis.2,4
Despite the relatively high incidence of cryptococcosis in SOT, no clinical trials have been conducted in this population and the treatment recommendations are extrapolated from studies in the population affected by HIV.4 As previously mentioned, the 2010 IDSA guidelines and 2019 guidelines of the American Society of Transplantation recommend an induction treatment based on a two-week association of L-AmB and flucytosine followed by consolidation and maintenance with fluconazole in meningeal or disseminated disease.2,4 However, nephrotoxicity, myelotoxicity and drug-drug interactions are frequent in the SOT population, which may require therapeutic adjustments. A treatment regimen with a single dose of L-AmB has recently been studied in patients affected by HIV, and we have successfully adapted this regimen for our SOT patient.3 We decided to give a second dose of L-AmB because the first dose had been well tolerated, in a patient with severe immunosuppression and an estimated high fungal burden: retrospectively, we can question whether a single-dose regimen could have been sufficient. More studies are needed to assess the safest and most effective antifungal regimen in SOT patients.
Another therapeutic challenge of cryptococcosis in SOT recipients consists of the management of immunosuppressive drugs. Reduction of the dosage of immunosuppressive drugs is recommended, although there is a concern for allograft rejection, as well as a risk of immune reconstitution inflammatory syndrome (IRIS), which can be severe. Up to 5–14% of SOT patients with cryptococcosis will experience IRIS, which appears most commonly 4–6 weeks after the initiation of antifungal therapy.7,13 CNS involvement and discontinuation of calcineurin inhibitors have both been associated with an increased risk of IRIS, in a retrospective study of 89 SOT patients with cryptococcosis. IRIS was associated with an increased risk of graft rejection.7 Interestingly, some studies have shown that calcineurin inhibitors act synergistically in vitro with antifungal agents against C. neoformans isolates, but this may occur at higher dosages than those usually prescribed.14 Expert opinion generally favors gradual reduction of corticosteroids and maintenance of calcineurin inhibitors.2,4,7
Conclusion
Cryptococcosis in SOT represents both a diagnostic and therapeutic challenge, as the clinical presentation is often non-specific and insidious, the risk for treatment adverse events is high and treatment guidelines specific to the SOT population are lacking. Disseminated disease should always be considered and an LP systematically done in all SOT patients presenting with cryptococcosis. Our patient presented with insidious symptoms, but already had a disseminated disease with fungemia. She was successfully treated with an induction regimen comprising two high doses of L-AmB (10 mg/kg) on day 1 and day 7, combined with flucytosine and fluconazole, followed by fluconazole consolidation and maintenance regimens. More studies are needed to assess the optimal antifungal therapy of cryptococcosis in SOT recipients.
Acknowledgments
The authors would like to acknowledge the work of the healthcare professionals at the Service of Pulmonology, the Department of Internal Medicine, the Service of Infectious Diseases and the Institute of Microbiology involved in the care of the patient.
Consent to participate
Informed consent could not be obtained from the patient as this case report was written after her death.
Availability of data and materials
All patient data that support this case report are included in the anonymized form in the published article.
Conflict of interest
The authors have declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Outside the submitted work, FL received research grants and/or speaker honoraria from Gilead, Pfizer, MSD, Mundipharma and Novartis. All fees were paid to his institution (Lausanne University Hospital).
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript. EG collected data from the patient’s records and wrote the initial manuscript. AK, FI, OM and FL have edited the manuscript.