


Background
Retinal venous pressure (RVP) is an important clinical parameter in the assessment of retinal blood flow. In the literature, there are only a few and discordant data on retinal pressure in healthy volunteers, as well as in patients with eye pathology, regardless of posture. A standard value study is intended to provide the current basics on the influence of posture on RVP. RVP is generally not lower than ambient intraocular pressure (IOP). Otherwise, the veins would partially collapse and blood circulation would stop. Current studies indicate that in most healthy people, RVP commonly equals IOP or lies slightly above it. Therefore, visible spontaneous venous pulsations (SVP) should be observed in most healthy eyes.1 However, an increased RVP has a significant influence on ocular perfusion pressure (OPP) which is the motor of blood circulation in organs. OPP is defined as the mean arterial pressure (MAP) minus RVP.2,3 Low OPP may be related to decreased MAP, increased RVP or both. RVP has been proven to be elevated in a variety of systemic and ocular diseases but especially in glaucoma patients.2,4–6
Glaucoma is one of the leading causes of irreversible blindness worldwide, representing up to an estimated 80 million people suffering from the disease by 2020.7 Current treatment strategies are meant to delay disease progression and do so by reducing IOP, one of the main risk factors for this disease. A high IOP automatically leads to higher RVP. This is particularly relevant in situations with markedly elevated IOP, such as in patients with acute angle closure glaucoma. However, in a significant number of patients, this IOP reduction alone is insufficient to halt or significantly decrease disease progression.8
Similarly, normal tension glaucoma (NTG) is considered a type of primary open angle glaucoma (POAG), but IOP is equal to or below the threshold (21 mmHg),9 suggesting that other factors may be involved in the pathogenesis of the disease. Actual studies suggest that an underlying vascular dysfunction or ocular blood flow disturbances in patients with glaucoma may further aggravate ganglion cell damage.2,10 Indeed, a vast literature demonstrates that patients with glaucoma and those with IOP within normal limits (so called NTG), have signs of ocular and systemic vascular abnormalities.4,11,12 Moreover, patients with glaucoma have a higher incidence of vascular-related clinical symptoms such as low systolic blood pressure,13 migraines14 and peripheral vasospasm.15
In recent years, studies have provided evidence of changes in IOP in different body positions.16–18 IOP elevation and progression of glaucoma associated with sleep positions suggest that there are similar risks of progression associated with sleep-related body postures adopted during non-sleep activities, such as reading, watching television and sunbathing. Posture-related management of patients with glaucoma, which is intended to reduce the risk or degree of progression, may include the use of specially designed pillows, bed-head elevation and recommendations to avoid postures that induce higher IOP.19
Blood pressure fluctuates considerably throughout the circadian period, with a clear decrease during sleep. This blood pressure dipping regularly exceeds 10% of the mean daytime values in normotensive and primary hypertensive subjects.20,21 Dipping seems to be important for cardiovascular health, and its disturbance accelerates the development of cardiovascular diseases. It is well known that the sleep-related blood pressure decline is the result of a downward shift of the baroreflex threshold. This threshold defines the blood pressure at which counterregulatory modulation of sympathetic nerve activity to the muscle vascular bed or the heart is initiated.15,22 A nocturnal increase in IOP and decrease in blood pressure leads to lower OPP, which may significantly increase the risk of glaucomatous visual field progression.
It is rather notorious that systemic hypertension accelerates atherosclerotic change inducing structural modifications of the arterial wall and reduction of vessel wall compliance. Many studies have proven a relationship between IOP and arteriosclerosis and its risk factors.20 However, rather surprisingly, at a given IOP, these factors do not or do not relevantly contribute to glaucomatous optic neuropathy (GON) Flammer Syndrome.22,23 A breakthrough in understanding the relationship between blood flow and GON came with the observation that a constant reduction of blood flow e.g. observed in subjects with arteriosclerosis, is quite well tolerated. If the reduction is marked, it can lead to so-called bland atrophy, but not GON.
As mentioned above, RVP in a healthy population is equal or slightly above IOP in the classical clinical setting in a sitting position (Figure 1). Therefore, it should be questioned whether retinal venous pressure increases in the supine position compared to the upright position and whether it has any difference between healthy volunteers and patients with ocular pathology.
_and_illustrative.jpg)
Methods
Study population
The total population of the prospective clinical study included 30 eyes of 11 patients and 15 healthy volunteers who were divided into two groups (Table 1): Group 1, healthy volunteers without any eye diseases (n=15) and Group 2, patients with known (or diagnosed) ophthalmological pathology (n=11). The control study groups were selected electively and carefully, encompassing individuals aged between 18 to 70 years.
Our hypotheses are that RVP may change with body position, depending on whether RVP is above or equal to IOP, and pressure in the retinal veins differs in the supine position, which leads to changes in blood flow. It should be noted that due to the nature of the method of investigation, no serious adverse events (AEs) and serious side effects are to be expected.
The participants were recruited via a flyer in the eye clinic and an advertisement in a daily press (Berner Zeitung Bund). We recruited healthy subjects and subjects with known ocular pathology with 18–70 years of age.
Study Design
Main parameter
The main parameter for the assessment was retinal venous pressure measured with the Ophthalmo-Dynamometer (Contactglass-Dynamometer according to Dr. Löw, Meditron, Völklingen, Germany). The observer evaluated the occurrence of pulsation of the veins on the retina by means of a gaze through an ophthalmic dynamometer. The digital display in mmHg of the ophthalmic dynamometer provides additive pressure for the objective determination of spontaneously existing retinal venous pressure. In this case, retinal venous pressure was measured as the primary parameter. And it was measured with an ophthalmo- dynamometer.
Secondary parameters
IOP and BP were measured as secondary parameters. IOP was measured with Goldmann applanation tonometry (GAT) and Perkins MK3 Tonometer (PAT). And the blood pressure is measured with digital automatic blood pressure monitor.
A) Goldmann applanation tonometry (GAT) is considered the gold standard for measuring IOP in the upright position due to its accuracy and reliability. By delicately flattening the cornea, it records the pressure needed for this flattening with remarkable accuracy. It is also preferred by investigators and patients alike for its ease of use and comfort. However, when measuring IOP in the supine position, the Perkins MK3 Tonometer (PAT) was the only feasible option available. The PAT yields IOP measurements that are closely comparable with GAT. Therefore, PAT is used in routine clinical practice, as part of the implementation of national guidelines, or preferred practice patterns, for glaucoma and ocular hypertension. This comparability between PAT and GAT highlights the practical utility of the Perkins tonometer, especially in situations where measuring IOP in the supine position is necessary or when the Goldmann device is not available. Several studies have demonstrated the close correlation between PAT and GAT measurements, underscoring the reliability of the Perkins tonometer in various clinical settings.24
B) Systemic Blood Pressure. Systolic and diastolic blood pressure (SBP and DBP, respectively) were measured using a digital automatic blood pressure monitor (boso-medicus prestige).
Measuring systemic blood pressure is necessary to calculate ocular perfusion pressure. As mentioned above, the mean OPP is defined as the mean arterial pressure minus IOP. Systolic and diastolic OPP can also be calculated using systolic and diastolic blood pressure values, respectively, minus IOP. Mean Ocular Perfusion Pressure (MOPP) = ⅔ (mean arterial pressure – IOP), where mean arterial pressure (MAP) = DBP + ⅓ (SBP – DBP).
C) Central Corneal Thickness. The central corneal thickness was measured using the SIRIUS corneal topography system.
From the time the ethics committee approved the study, 11 patients with known ocular pathology and 15 age-matched healthy subjects were recruited by means of a flyer in the Augen Zentrum Fankhauser in the time span of 3–6 months. Each subject was asked to sign an informed consent form before entering this study. The content of this information is documented in the declaration of consent. The subject is informed if there are significant new findings on the test medication during the study. The consent of the subject to participate in the clinical study is given with the date and signature of the subject, as well as the investigator. A copy of the signed subject information and a copy of the declaration of consent were provided to each subject. The second copy was kept by the investigator. It was specifically pointed out that no studies could be carried out until a legally valid declaration of consent had been provided by the subject. The study and its course were explained to the interested party. After the consent was signed, the potential test person was asked to participate in the investigation.
Subjects could be admitted to this study after signing the informed consent form, which described the procedure as follows.
The complete procedure is non-invasive and non-injurious or penetrating. At the beginning, the intraocular pressure is determined using the Haag-Streit Goldmann applanation tonometer BQ/900 in the upright position (Figure 2).
.png)
The central corneal thickness is then measured using the SIRIUS corneal topography system. After application of the local anesthetics (Oyxbuprocain or Tetracaine eye drops), the contact lens dynamometer, along with a contact fluid-gel (Methocel 2%) is placed gently on the cornea. Digital Ophthalmo-Dynamometry by Dr. Loew (Meditron, Germany) consists of a three-mirror Goldmann lens with a ring-shaped attachment containing several precision sensors affixed to the rear. The sensors continuously measure the force exerted by the ophthalmologist on the eye using a contact lens. The contact lens dynamometer is connected by a thin, flexible cable to a central unit approximately equal to the size of the handheld calculator. A liquid crystal display shows the delta pressure in mmHg based on the calibration curve.
The measurements were conducted with a slit-lamp microscope (Haag Streit BQ/900) in the upright position und with MR3/Meridian (Bern Switzerland) in the supine position. The pressure increases until one of the segments of veins on or close to the optic nerve head started to pulsate, and the required pressure is calculated as the sum of the ocular dynamic force (OFD) and IOP. Due to the difficulty of visualizing the retinal veins, mydriatic eye drops are used to dilate the pupil.
RVP and IOP were measured first in the upright position (Figure 3). The examination in the supine position was performed 15 minutes after lying down.
_by_an_ophthalmodynamometer.png)
The duration of the measurement per subject was 120 min. Until now there have been no actual experimental data on the effect of postural change on RVP. The cancellation criteria were adverse events (AEs) and side effects (adverse reactions [AR]). The usage of the eye drops is carried out by the investigator. All examinations are painless, the eyes are externally touched and the pupils dilated, as required. For the complete study, it is planned to submit the evaluation and report to the ethics committee, approximately 6–9 months after the approval of the ethics committee.
Effectiveness evaluation
The purpose of the study was to determine the actual condition of the venous pressure by changing the posture of the subject in a prescriptive manner.
The standard deviation of the interindividual distribution of IOP is well known to be around 2.5 mmHg. It is fair to assume that the standard deviation of RVP in healthy subjects is approximately the same but may be twice as large in glaucomatous eyes in either posture, although we cannot know exactly without anticipating the results of the present study. We attempted to achieve a standard error of the mean RVP of approximately 0.5 mmHg in all four situations considered here (normal and glaucomatous eyes, both positions). From the figures just indicated, the number of participants is estimated to be between 25 and 100. It was decided to carry out the study with 50 participants in both groups, admitting that the final accuracy may deviate slightly from the indicated goal.
Statistical analysis
Group characteristics are presented as means, standard deviations (SD), medians, interquartile ranges (IQR) and percentages for categorical variables. RVP and IOP are described as means and SD, as well as graphically with boxplots. A t-test was performed to compare the groups and postures.
To test the effect of posture on RVP a regression analysis was performed using mixed model. Sex, age, diastolic blood pressure and IOP were included to reduce variation and to consider possible confounders. The person is considered a random variable:
rvp∼sex+age+iop+bp_diast+group+posture+group:posture+(1|subject_id).
The variable group categorizes individuals into two groups: volunteers and patients, with posture acting as the additional factor, comparing the effects of supine versus upright positions. Group: posture indicates if there is an interaction effect between group (voluntary/patient) and posture. Statistical analysis was performed with R (R version 4.2.1, 2022–06–23).
Results
The COVID-19 pandemic caused major disruptions in our project. We decided to share the marbled result with the scientific community as it has important implications for understanding retinal blood flow and therefore contributes to the knowledge about the pathogenesis of glaucoma.
Of the 26 persons included in the study, 15 (58%) were volunteers and 11 (42%) were patients, with a mean age of 57.7 years (SD, 12.5) and 55.7 years (SD, 10.3), respectively. Table 2 displays the distribution of sex and age among volunteers and patients.
Table 3 compares the vital parameters of the volunteers and patients. Patients had an average of 10.0 mmHg (p=0.002) higher ophthalmodynamometric force (ODF) than the volunteers. There was no significant and relevant difference between the patients and volunteers in terms of systolic and diastolic blood pressure and IOP. RVP in patients was 9.2 mmHg higher than that in volunteers, but the difference was not significant (p=0.756).
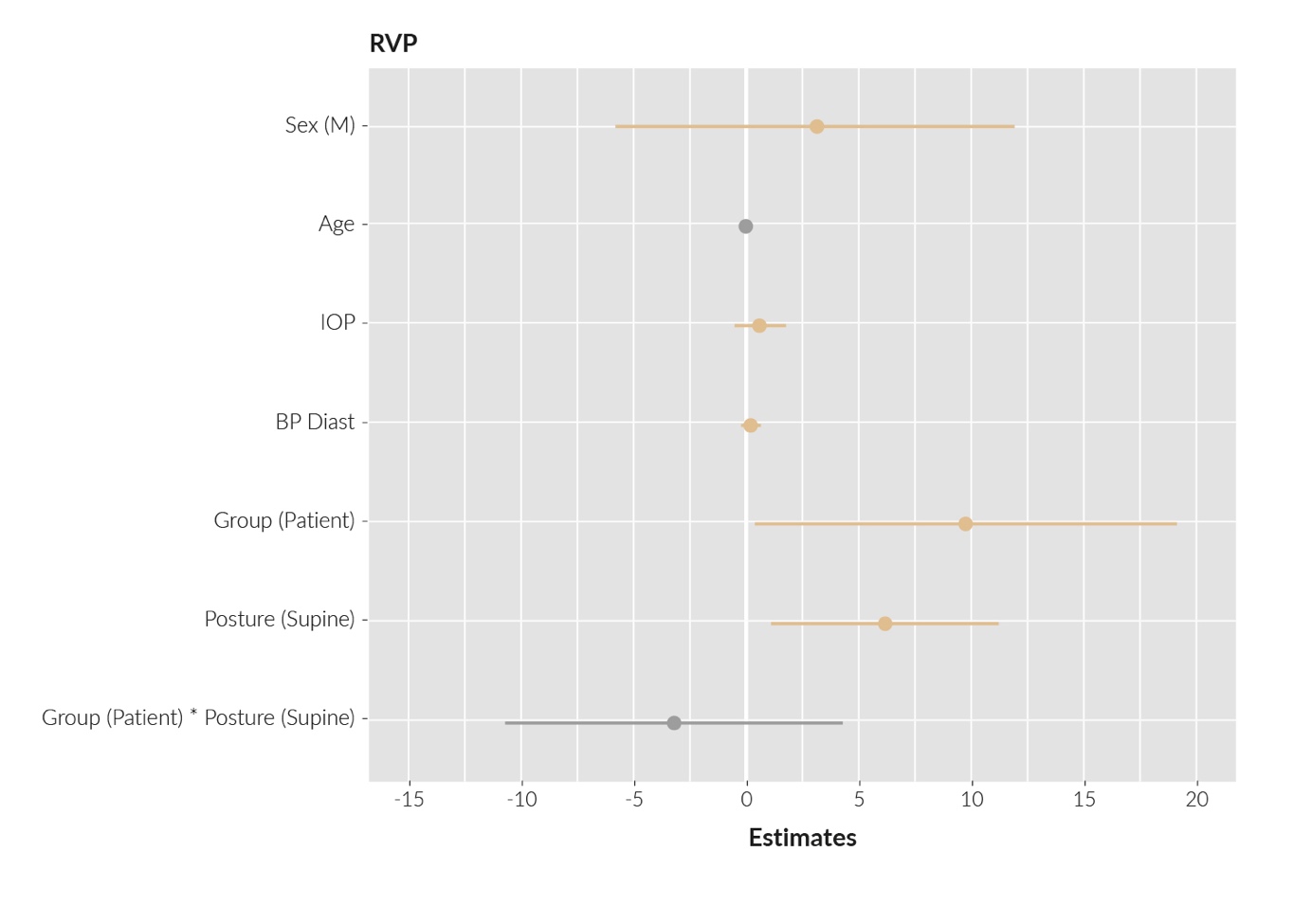
The results from the regression analysis (Table 4 and Figure 4) showed that there was a difference in RVP between supine versus upright positions of 6.06 mmHg (95% CI: 1.02–11.10; p=0.020). Patients had a 9.66 mmHg higher RVP (95% CI: 0.30–19.01; p=0.043) than the volunteers. There was no difference in RVP according to sex, age, IOP or blood pressure. There was a small interaction effect between the group and posture of -3.29 mmHg (95% CI: -10.80–4.21; p=0.381), but the difference was not statistically significant.

Discussion
The higher RVP of 9.66 mmHg (95% CI: 0.30–19.01; p=0.043) in patients compared to volunteers can be explained by potential underlying factors influencing retinal venous pressure, such as variations in ocular health conditions, alterations in vascular resistance or disparities in intraocular pressure regulation mechanisms between the patient and volunteer groups. This indicates a potential association between ocular pathology and elevated venous pressure. This observation aligns with those of previous studies, highlighting the impact of underlying ocular conditions on retinal hemodynamics. This suggests plausible factors related to compromised venous outflow, altered vascular resistance or variations in intraocular pressure regulation mechanisms that could contribute to this disparity.
The supine position had an RVP which was 6.06 mmHg higher (95% CI: 1.02–11.10; p=0.020) than that in the upright position. This applies for both patients and volunteers, suggesting a shared response to postural changes regardless of ocular health status, age or gender, affirming the universality of the observed impact on retinal venous dynamics. This finding is in line with existing literature emphasizing the influence of postural changes on RVP, indicating potential implications for ocular perfusion dynamics across different positions. In a few cases, healthy subjects showed high IOP and high RVP. According to history, they were healthy people, but we cannot rule out that there were also participants in the healthy group who suffered from unrecognized diseases. Autoimmune diseases are associated with a high RVP.
One limitation of the study is that the design was not random. Both patients and volunteers were enrolled by asking participants to self-report their medical history, which may have caused a selection bias. The small number of people results in low power, which may mask the real effects. For example, the interaction effect between group and posture, which was not significant, may be caused by the small sample size.
This study was conducted in response to the lack of published solid data using RVP to assess the status of retinal blood flow considering the positioning of the patient.
The data statistics and analysis presented in this study indicate a strong association between RVP and posture. The data show an increase in RVP for patients in the supine posture compared to the subjects in the upright position.
We recommend extending this study to include additional quantitative parameters. Fluid (blood) viscosity measurements and imaging are among potential cases. Viscosity could be an indicatior of the pathological status of IOP, and thus RVP. For imaging, we suggest using Optical Coherence Tomography (OCT). These will boost the measured data in a stronger quantified manner, supported by imaging. Such extension of the study may provide deeper insights into the interplay between RVP, ocular pathologies and the influence of positioning, further contributing to the understanding of retinal hemodynamics and its clinical implications.
The small sample size also limits the statistical power, potentially masking real effects, such as the interaction between group and posture.
In conclusion, this study addresses a gap in the literature by providing valuable insights into the role of RVP in assessing retinal blood flow with respect to patient positioning. The statistical analyses performed indicate a robust association between RVP and posture, notably observing increased RVP among patients in the supine position compared to upright subjects.
Acknowledgments
I must first extend my sincerest gratitude to my family. I am indeed deeply thankful to my wife, who supported me all along this way during the past years.
To conclude, I cannot forget to thank my mother and my brother Ashraf Fetian for supporting me during the compilation of this dissertation.
I am eternally grateful to my uncle Dr Issa Fitian, who always encouraged me to go on and reassured me that this work will be valuable and dignified.
I thank my friends in Basel for cooperating with me and presenting as volunteers during the training period before the start of the project.
The authors would like to express our deepest appreciation to Fabio Valeri and Stefan Zechmann for supporting us with the data bank program. The authors thank the Schwickert-Stiftung, Switzerland, for granting financial support to the research project.
Ethics approval and consent to participate
General written consent was obtained from the patients for the publication of this study and any accompanying images. The study protocol was approved by the Ethics Committee (BASEC ID: 2017-01795) and adhered to the principles outlined in the Helsinki Declaration.
Availability of data and materials
All patient data that support this study are included in anonymized form in the published article.
Conflict of interest
The authors have declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript. IRF collected the data and wrote the manuscript. IRF also served as the project coordinator, contributing to the main scientific ideas and hypotheses presented in the manuscript, proofreading and making corrections. HB initiated the statistical ideas, while VF performed the statistical analysis. MB and MM formatted the manuscript, inserted references and assisted with illustrations and data collection. FF and JF provided expertise in measurements and data collection and analysis. IRF recruited patients, analysed data and assisted in drafting the manuscript. All authors have reviewed and approved the final manuscript.