
Introduction
Since the first antiretroviral therapy (ART) was approved by the US Food and Drug Administration (FDA) in 1987, improvements in ART have resulted in fewer side effects and a greater and more rapid reduction in human immunodeficiency virus (HIV) viral load. Furthermore, for most people living with HIV (PwH), the pill burden has been reduced to one single tablet per day.1 In more recent years, the treatment paradigm of simply attaining viral suppression has shifted, with HIV therapy considered successful when PwH not only achieve sustained viral suppression but also when their health-related quality of life (HRQoL) remains consistently high. A holistic, long-term and patient-centric treatment approach achieves this.2,3
The attainment of such ambitious treatment goals requires robust combination ART such as bictegravir/emtricitabine/tenofovir alafenamide (BIC/FTC/TAF).4 The INSTI-based single-tablet regimen (STR), Biktarvy® (BIC/FTC/TAF), can meet the high demands of a contemporary ART.5 BIC/FTC/TAF is taken once daily, with or without food,6 and is indicated[1] in Switzerland for the treatment of HIV type 1 (HIV-1) infection in treatment-naive adults or as a replacement for the current antiretroviral therapy.7
The effectiveness and tolerability of the BIC/FTC/TAF regimen in long-term clinical practice is increasingly supported by emerging data. Data at 36 months from the BICSTaR cohort were recently published, examining the use of BIC/FTC/TAF in a diverse group of treatment-naive and treatment-experienced participants in clinical practice.8,9 This data was discussed during the 11th German-Austrian AIDS Congress (DÖAK) by a group of eight experts from Germany, Austria, and Switzerland (DACH). Each of the experts summarized one specific topic, which were combined and presented in this paper. Key take-home points relating to the longer-term BICSTaR data discussed during this meeting are summarized here, as well as the clinical experience of the experts with BIC/FTC/TAF and its impact on long-term treatment success.
A holistic approach to care
Nowadays, successful HIV therapy goes beyond suppressing viral load. It focuses on holistically assessing long-term treatment success.10 This includes long-term effectiveness and tolerability without the risk of resistance development, as well as immune system protection, minimal drug-drug interactions (DDIs) and improved quality of life.2,3,10 Overall, it is essential to consistently prioritize the health-related needs of PwH, utilizing an individual and patient-centered approach throughout their lifelong therapy journey (Figure 1).10

BICSTaR study design
The BICSTaR study is an ongoing, prospective, multinational, non-interventional cohort study encompassing five cohorts with approximately 2,500 participants.8,9 Most participants were enrolled in European countries such as Germany, France, Italy and Spain. Additionally, cohorts from Canada, Israel, Japan and other Asian countries were investigated. The interim analysis, presented by Schellberg et al. at DÖAK, included pooled data collected up to August 2022 in 781 participants (Canada: 177; France: 213; Germany: 391).8 The study included both ART-naive (TN) and treatment-experienced (TE) adults living with HIV.8,9 The main study is designed for two years. Participants from Canada, France and Germany were offered the option to transfer to a three-year extension phase after completing the two-year main study.11 At the start of the main study, the majority of participants were male (87% TN and 86% TE), with median ages of 39 and 49 years, respectively. In the TN group, 26% of participants were aged ≥50 years, while the percentage in this age group reached 48% among TE adults.11
Furthermore, a high proportion of participants had comorbidities (53% TN and 73% TE), with neuropsychiatric disorders being the most common (18% and 29% in the TN and TE groups, respectively). Approximately one-fifth of TE participants had hyperlipidemia (20%) or hypertension (19%). At the start of the study, 92% of TE subjects had a viral load (HIV-1 RNA) of <50 copies/mL. The median CD4 cell count was 424 cells/µL and 657 cells/µL in the TN and TE groups, respectively. Change from baseline in CD4 cell count at 24 months was 681 cells/µL (median change +228 cells/µL) and 704 cells/µL (median change +48 cells/µL) in TN and TE groups, respectively. Among TN participants, 27% had a late-diagnosed HIV infection (CD4 cells <200 cells/µL and/or an AIDS-defining illness at baseline).11
Long-term efficacy of BIC/FTC/TAF is high
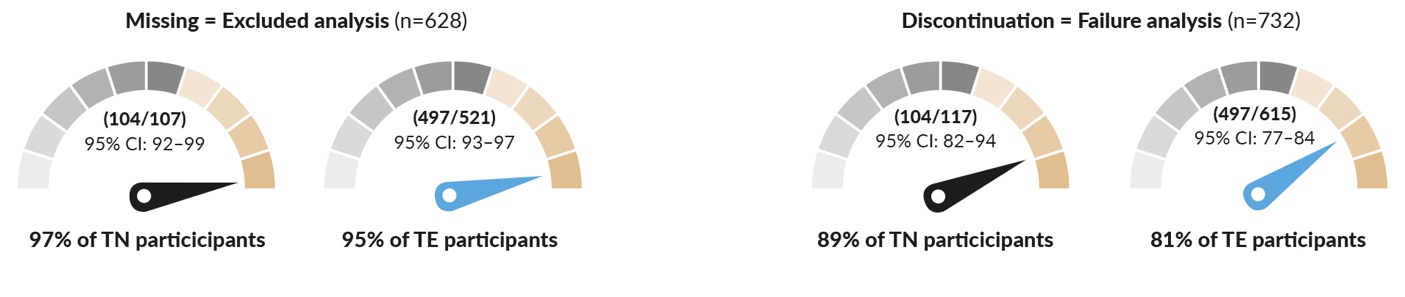
The basis for long-term treatment success remains sustained viral suppression, a goal achieved in almost all participants receiving BIC/FTC/TAF. At the end of the main study (24 months), 97% of TN and 95% of TE participants had achieved virological suppression (viral load <50 HIV-1 RNA copies/mL) in a missing = excluded analysis (i.e., participants for whom no data are available were consistently excluded) (Figure 2).11 Additionally at the end of the main study period (24 months), virological suppression had been achieved by 89% of TN participants and 81% of TE participants, as determined by a discontinuation = failure analysis, meaning any participants who stopped taking BIC/FTC/TAF for any reason during the study were considered as treatment failures.11
_after_24_months_in_treatment-n.jpeg)
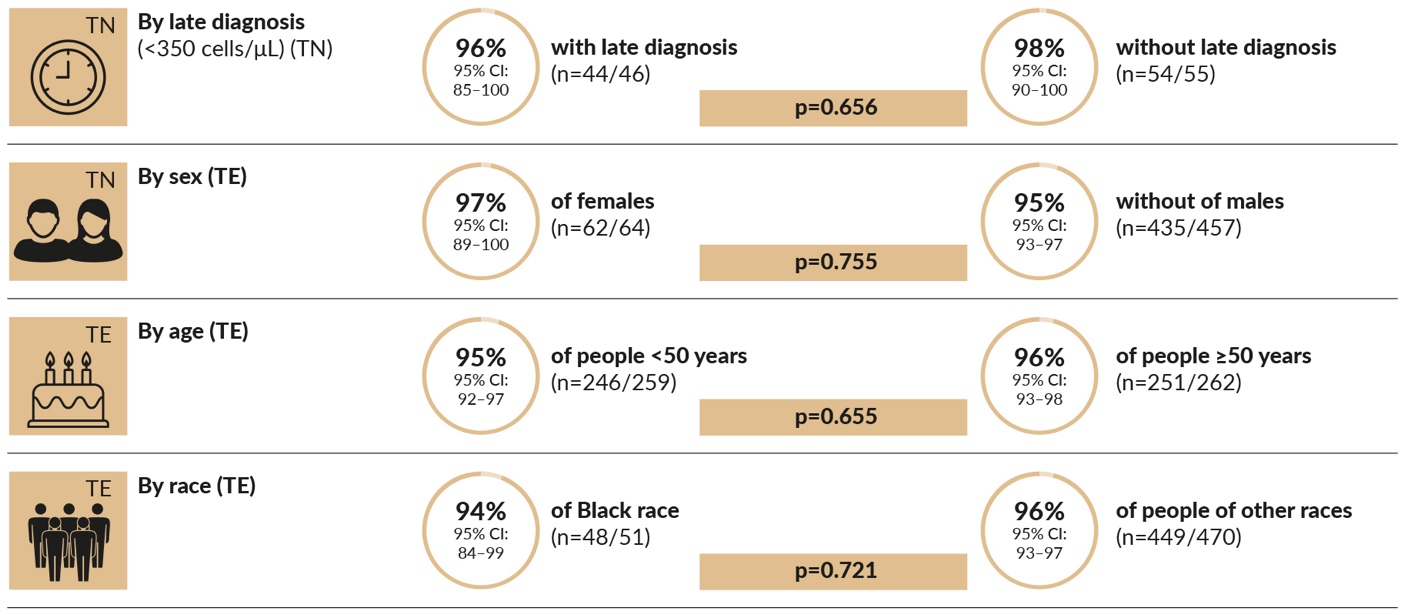
Gender, age, ethnic background, and the timing of diagnosis had no influence on the study outcome (Figure 3).12

Consistent results after 36 months
One critical component to achieving sustained undetectable viral load is ensuring that ART regimens can provide rapid and durable viral suppression.13 At the 11th German-Austrian AIDS Congress DÖAK 2023, a pooled interim analysis after 36 months (24 months from the main study and 12 months from the extension phase) was presented. Data from 781 participants across Canada, France and Germany demonstrated the sustained virological and immunological efficacy of BIC/FTC/TAF. At 36 months, 97% of both TN and TE participants exhibited viral loads of less than 50 HIV-1 RNA copies/mL (Missing = Excluded analysis [M=E]; i.e., participants for whom no data are available were excluded from the analysis) (Figure 4).8
In the overall population, including participants who had either discontinued the study or the study medication, the virological suppression rate was 76% and 78% for the TN and TE groups, respectively (Discontinuation = Failure analysis [D=F]; i.e., participants who discontinued BIC/FTC/TAF during the study period for any reason were considered as treatment failures) (Figure 4).8 BIC/FTC/TAF also demonstrated a high resistance barrier in real-world clinical practice, with no treatment-emergent resistance to any of the components.8 Furthermore, this cohort showed significant improvements in CD4 cell count (+232 cells/μL in the TN group [p<0.001] and +44 cells/μL in the TE group [p<0.001; Wilcoxon signed-rank test]), as well as in the CD4/CD8 ratio (+0.5 [p< 0.001] and +0,06 [p<0.001; Wilcoxon signed-rank test] in TN and TE participants), respectively (note: participants for whom data were available at the study’s start and after three years were included).8 These overall positive data align with the results of clinical and other real-world studies with BIC/FTC/TAF published in recent years.14

BIC/FTC/TAF was well-tolerated
Simple patient and therapy management and the best possible HRQoL are crucial for long-term treatment success.10,15 To achieve this, the tolerability of ART plays a crucial role. BIC/FTC/TAF has also demonstrated good tolerability in real-world clinical practice, with most drug-related adverse events (DRAEs) documented in the first six months.8
An interim analysis after three years of data from the German subpopulation of the extension phase of the study revealed that 17% (n=67/391) of participants experienced DRAEs. Two participants experienced severe DRAEs, both of which were depression. The most common DRAEs in the overall German population were weight gain (4.6%), depression (2.6%), fatigue (1.8%), diarrhea (1.3%) and nausea (1.3%).9 The distribution of DRAEs was comparable between TN and TE participants. Moreover, BIC/FTC/TAF was well-tolerated overall, and no specific side effects were linked to an increased discontinuation rate or a preference to change treatment. In the TN group there were 7 BIC/FTC/TAF discontinuations: DRAE (n=5), participant decision (n=1), non-drug related adverse event (n=1), whereas in the TE group there were 61 BIC/FTC/TAF discontinuations: DRAE (n=29), pregnancy (n=1), lack of efficacy (n=4), participant decision (n=7), investigator discretion (n=5), non-drug related death (n=6), new treatment available (n=3), and non-drug related adverse event (n=6).9
For those participants with a DRAE of weight increase, 7/9 (78%) TN and 9/22 (41%) TE participants experienced weight gain ≥ 10% at any point up to 3 years.16 The weight changes (calculated from the median individual participant changes from baseline to 3 years) observed in TN participants were mainly attributed to the “return to health” effect. In TE individuals, the weight change was primarily driven by the switch from TDF (tenofovir disoproxil fumarate) to TAF; adults with an HIV infection who switched from another TAF-based regimen to BIC/FTC/TAF experienced a median weight gain of 2kg over three years,9 corresponding to values observed in the general population.17–19
High persistence of the BIC/FTC/TAF regimen
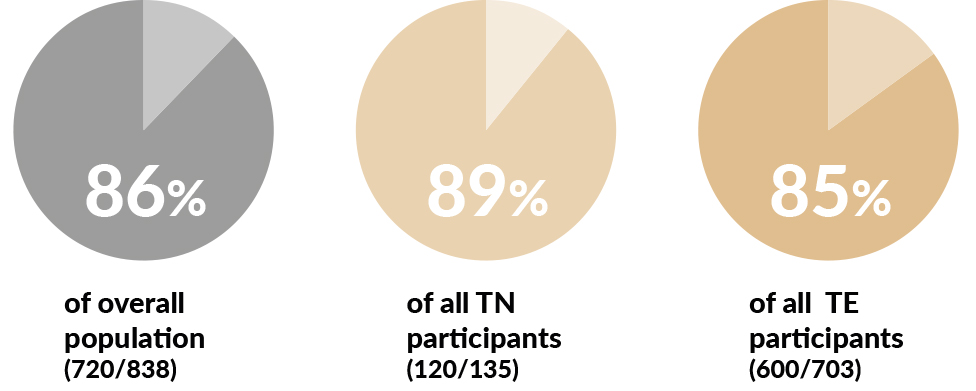
The good tolerability of BIC/FTC/TAF was reflected by its high persistence: after 24 months, over 86% of participants continued to take BIC/FTC/TAF (Figure 5).12
_th.jpg)
Patient perspective
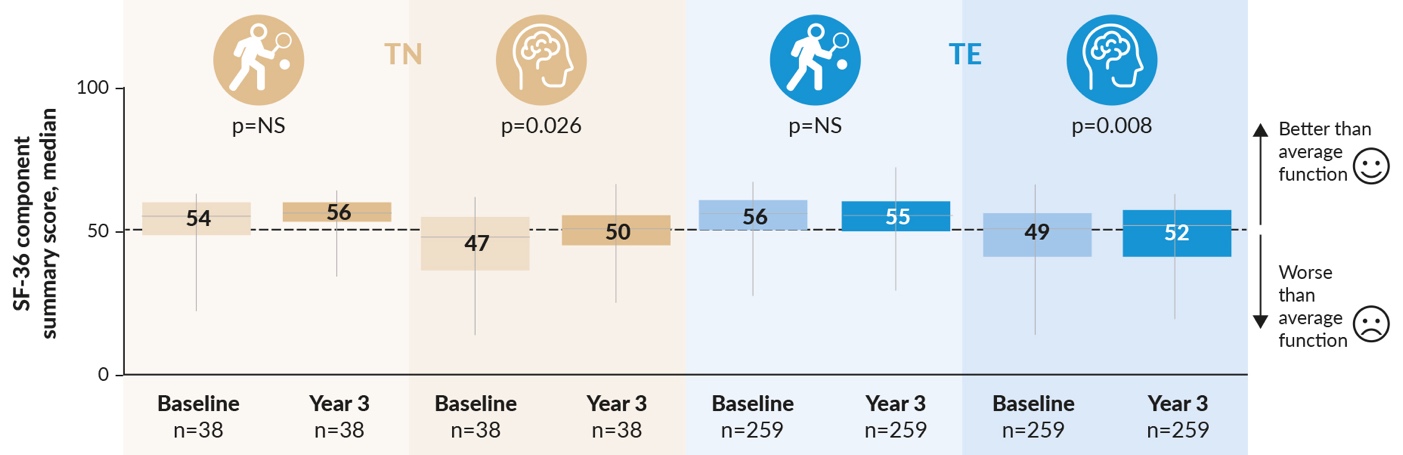
Treatment outcome from the patient’s perspective is essential, along with the efficacy and safety of a regimen.20 Thus, an important aspect of the pooled interim analysis after three years (involving participants from Canada, France, and Germany) was Patient Reported Outcomes (PROs). In TN individuals, the distressing symptoms, as determined by the HIV Symptom Index (HIV-SI), significantly decreased with BIC/FTC/TAF (p=0.002) and remained stable in TE individuals. Additionally, participants benefited from BIC/FTC/TAF therapy in terms of improved physical and mental HRQoL components (Figure 6).8
_therapy_improves_the_com.jpeg)
A total of 118 (8%) participants in the TN group had at least one primary mutation at baseline: non-nucleoside reverse transcriptase inhibitor (NNRTI) mutation (4%), protease inhibitor (PI) mutation (2%), nucleoside reverse transcriptase inhibitor (NRTI) mutation (2%). In the TE group, a total of 617 (12%) participants had at least one primary mutation at baseline: NNRTI mutation (6%), PI mutation (2%), NRTI mutation (6%), integrase strand transfer inhibitor (IINST) mutation (<1%).8 At study entry, 2 of 122 TN patients had the NRTI mutation M184V, of which one patient was not eligible for the extension phase, compared to 66 TE patients with M18V or M19l mutations (41 and 25, respectively).16 Satisfaction with therapy, as determined by the HIV Treatment Satisfaction Score (HIVTSQC), was significantly increased in TE individuals within 12 months after switching to BIC/FTC/TAF (a median increase of +24 out of a maximum of +30 achievable points; p<0.001).21
High suitability of the BIC/FTC/TAF regimen for everyday use
There was a consensus among the experts that the real-world data from the BICSTaR study reflect the high practicability of BIC/FTC/TAF. For example, factors like unclear prior therapies or hepatitis B virus (HBV) status typically do not play a role in the efficacy and tolerability of this STR.22
While the BICSTaR study is representative of most PwH seen in clinical practice, certain groups are still underrepresented, including PwH with very low CD4 counts or opportunistic infections and with substance abuse disorders. However, according to the experts, BIC/FTC/TAF therapy also works well for these people; the provider’s personal experience will play a significant role in successfully managing these PwH. The number of PwH engaged in chemsex is increasing significantly, and these individuals often face severe life issues.23 Omitting ART dosages is also frequently observed within this group. Overall, therapy with BIC/FTC/TAF has been observed to work well even for individuals involved in chemsex who typically lead unconventional, disordered lives.24,25
Adherence to the regimen is crucial
The topic of adherence was among the important aspects discussed during the DACH expert meeting. The consensus was that achieving high treatment adherence requires personalized patient care, with the extent of necessary support varying greatly depending on the PwH’s individual circumstances. The rapid decrease in viral load at the beginning of ART can motivate PwH to continue therapy and should be demonstrated to them repeatedly. According to the authors’ experiences, adherence may not apply equally to all medications. For example, there may be differences in adherence to ART compared to other treatments for the same individual. Other PwH may come for appointments regularly but do not consistently take their ART. For example, in the case of a young male patient who engaged in chemsex, the computer software at the practice revealed that this individual had collected too few prescriptions without being aware of his non-adherence. However, this was not reflected in his lab results.
Reasons for the non-adherence mentioned above can be numerous, such as substance abuse or changes in life circumstances. Therefore, discussing the patient’s life situations and needs during a trusting conversation is important.26,27 A structured and regular questioning process is necessary to assess adherence. PwHs with biographical disruptions require a robust regimen like BIC/FTC/TAF.
The increasing importance of comorbidities and concomitant medications
Modern ART has significantly contributed to reducing mortality in PwH and aligning life expectancy with people living without HIV.28 Accordingly, the proportion of adults living with HIV who are 60 years and older is increasing.29 With the aging of PwH, the incidence of comorbidities such as hyperlipidemia, hypertension or diabetes increases.30 Furthermore, with the increasing number of comorbidities and/or concomitant medications, the issue of drug interactions between ART and other drugs becomes increasingly important.
BIC/FTC/TAF has few DDIs.31,32 Clinically, the most relevant DDIs with BIC/FTC/TAF are with moderate or strong CYP3A/UGT1A1 enzyme inducers (e.g., St. John’s Wort, rifampicin or rifabutin), as well as polyvalent cations. Magnesium and other polyvalent cations should be taken two hours apart from BIC/FTC/TAF.6 Regarding polyvalent cations, many PwH often consume “protein products” for the gym or juices with mineral supplements without realizing that they often contain a high amount of calcium and sometimes undisclosed additives. Therefore, there is a need to educate PwH accordingly.
To assess the DDI risk of an ART, the authors recommended using the EACS Guidelines33 or the University of Liverpool’s Interactions Checker.31 With regard to potential DDIs, the preference for unboosted regimens can also facilitate patient care.
Therefore, the treatment plan for PwH aged over 50 should be adjusted. Before starting treatment, emerging comorbidities should be considered, and the ART regimen should be selected accordingly.
Conclusion/take-home messages
Beyond sustained viral suppression, life circumstances and health-related needs of people living with HIV should be prioritized. In addition, an individual and patient-centered approach should be employed for people living with HIV throughout their lifelong therapy journey. Real-world data from the BICSTaR study confirm the findings from clinical trials on BIC/FTC/TAF in a broad patient population. Thus, therapy with BIC/FTC/TAF supports long-term treatment success, aiming for a holistic, long-term and patient-specific treatment approach to provide the best possible HRQoL for adults living with HIV.
Consent for publication
General written consent was obtained from the patient for the publication of this study/case report and any accompanying images.
Availability of data and materials
All patient data that support this study/case report are included in anonymized form in the published article.
Conflict of Interest and Funding
All authors received honoraria for participating at the expert group discussion at the German-Austrian AIDS Congress (DÖAK). No honoraria was received for the writing of this manuskript. In addition, the authors declare the following conflicts of interest: CM received speaker fees/honoraria from Gilead Sciences, MSD, Pfizer and ViiV Healthcare. SVS received personal fees from Abbvie, BMS, Gilead Sciences, Janssen, KrewelMeuselbach, MSD, Pfizer, Thera Technologies and ViiV Healthcare. STS received personal fees from Abbvie, Cepeid, Gilead Sciences, GSK, Janssen, MSD and ViiV Healthcare. CS received consultation/speaker fees and travel support to conferences from AbbVie, Gilead Sciences, Janssen, MSD and ViiV Healthcare. CW received consulting fees/honoraria from AbbVie, AstraZeneca, Gilead Sciences, GlaxoSmithKline, Janssen, MSD, Pfizer, Roche and ViiV Healthcare. AZ received honoraria from Gilead Sciences for advisory boards and clinical studies. WB received personal fees and/or travel grants from AbbVie, Gilead Sciences, GSK, Takeda and ViiV Healthcare. CB received grants and personal fees from Gilead Sciences and ViiV Healthcare for travel sponsorship and consultation.
Funding
The publication costs for this article were financially supported by Gilead Sciences Switzerland Sàrl.
Author contributions
All authors contributed to the reviewing of the draft of the manuscript and approved the final manuscript. CW, CS, STS and SVS were involved as active sites for the BICSTaR real-world study. STS summarized the study design and general concept of the BICSTaR real-world study. CW and CS recapitulated the efficacy results and safety results of the study, respectively. SVS summarized the patient-reported outcome results of the BICSTaR real-world study. CB outlined the management of PLWH with difficult ARV adherence. CM summarized the drug-drug interaction profile of BIC/FTC/TAF. WB and AZ contributed two relevant patient case reports.
Biktarvy is indicated for the treatment of human immunodeficiency virus type 1 (HIV-1) infection in treatment-naïve adults, or to replace current antiretroviral therapy in patients - who have not had a history of virological treatment failure, and - who have been virologically suppressed with stable antiretroviral therapy for at least 6 months (HIV-1 RNA <50 copies/ml), and - in whom HIV-1 mutations against the class of integrase inhibitors, emtricitabine or tenofovir have not been detected at any time.